Ohio Gov. Mike DeWine has officially asked the Centers for Medicare and Medicaid Services to approve Medicaid work requirements.
Under the proposal, Ohio Medicaid expansion recipients would need to be at least 55 years old, employed, be enrolled in school or a job training program, be in a recovery program, or have a serious physical or mental health illness.
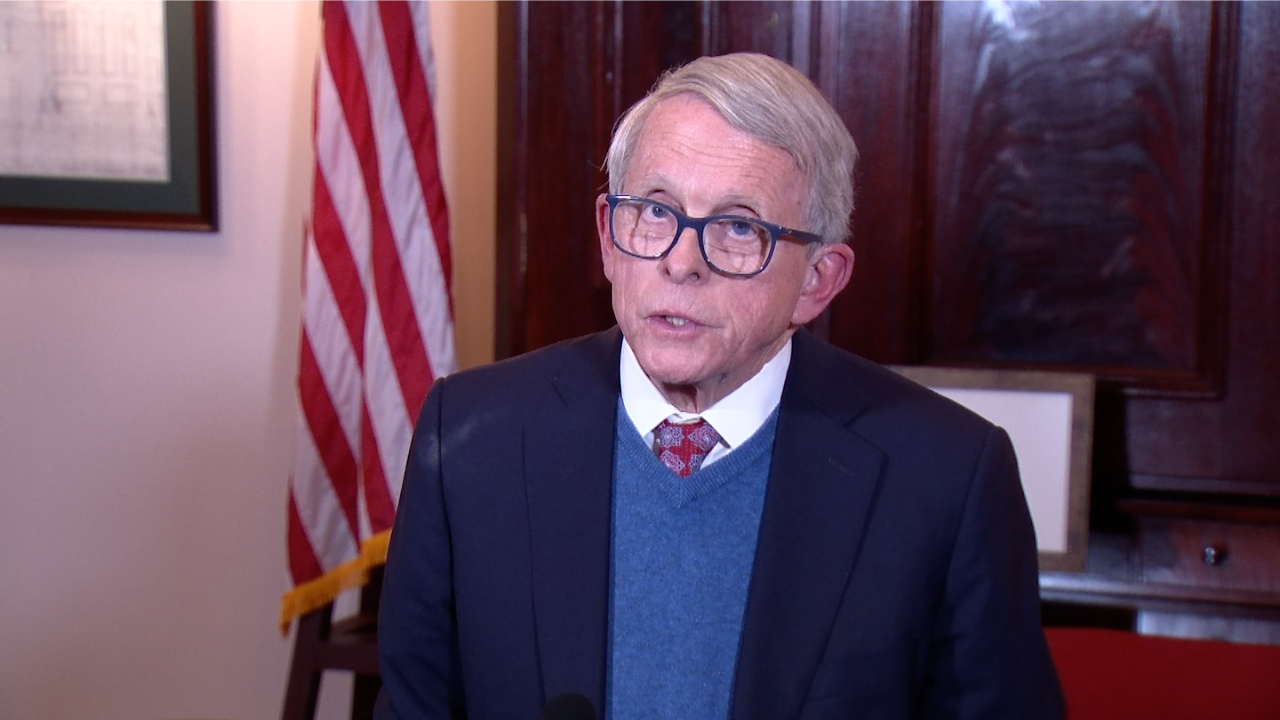
“As part of our work to empower people to reach their full potential, we have a responsibility to make sure as many Ohioans as possible are on a pathway toward financial independence,” DeWine said in a statement. “Reinstating our work requirement will promote self-sufficiency, it will give more people the purpose and pride that comes with a job, and it will improve the well-being of Ohio’s workforce.”
Medicaid offers health coverage to households making at or below 138% of the poverty line — $44,367 a year for a family of four. About 92% of U.S. adults under age 65 and eligible for Medicaid are already working or are exempt from requirements due to caregiving responsibilities, illness or disability, or school attendance, according to the Kaiser Family Foundation.
DeWine sent a letter to Health and Human Services Secretary Robert F. Kennedy, Jr. asking to approve the work requirements on Friday. Ohio House Speaker Matt Huffman and Ohio Senate President Rob McColley also signed the letter.
The Centers for Medicare and Medicaid will now review Ohio’s waiver and then the federal agency will have a 30-day comment period, said Ohio Department of Medicaid Spokesperson Stephanie O’Grady.
Once those steps are completed, Ohio’s Medicaid department will begin talks with the federal agency about setting up state terms and conditions, O’Grady said.
“We are dedicated to delivering high-quality healthcare to millions of Ohioans every day, empowering them to take control of their own health,” ODM Director Maureen Corcoran said in a statement. “By encouraging them to seek employment, we not only enhance their quality of life, but also contribute to healthier communities and a thriving economy in Ohio.”
Ohio’s 2023 budget requires the state Medicaid department to re-apply with the federal government under the new presidential administration for permission to impose work, drug testing, and/or education requirements for adult Medicaid health coverage recipients.
ODM received more than 450 comments on the proposed Medicaid work requirements and an overwhelming majority opposed the requirements with many sharing about their personal experiences with Medicaid.
Megan Henry is a reporter for the Ohio Capital Journal and has spent the past five years reporting in Ohio on various topics including education, healthcare, business and crime. She previously worked at The Columbus Dispatch, part of the USA Today Network.
Ohio Capital Journal is part of States Newsroom, the nation’s largest state-focused nonprofit news organization.
The committee was designed to reduce barriers to care for people of color, LGBTQ+ people and rural Americans. A new executive order deemed it “unnecessary.”
President Donald Trump has directed the Centers for Medicare and Medicaid Services (CMS) to disband a committee to identify and reduce systemic barriers that people of color, LGBTQ+ people and rural Americans encounter when trying to access government health care programs.
The directive came as part of an executive order on “commencing the reduction of the federal bureaucracy.”
Trump directed the heads of relevant agencies to disband within two weeks entities that include the Health Equity Advisory Committee at CMS, the Advisory Committee on Voluntary Foreign Aid at the U.S. Agency for International Development, the Community Bank Advisory Council at the Federal Deposit Insurance Corporation, and Secretary’s Advisory Committee on Long COVID at the Department of Health and Human Services.
“It is the policy of my Administration to dramatically reduce the size of the Federal Government,” Trump wrote in the order. “This order commences a reduction in the elements of the Federal bureaucracy that the President has determined are unnecessary.”
The establishment of the CMS Health Equity Advisory Committee was prompted by an executive order “On Advancing Racial Equity and Support for Underserved Communities Through the Federal Government” that Democratic President Joe Biden signed on his first day in office.
Xavier Becerra, the head of the Department of Health and Human Services under Biden, published the committee’s charter in July 2024, with the stated goal of making “recommendations on the identification and resolution of systemic barriers in the CMS programs that hinder access and quality for beneficiaries and consumers.”
The committee’s purview included Medicare, the government health insurance program for the elderly and disabled; Medicaid, the government health insurance program for lower-income Americans; the Children’s Health Insurance Program (CHIP) for children from low-income families; and the marketplace of health insurance programs established by the Affordable Care Act. Its mandate included addressing systemic barriers to access that included structural racism, which Trump labeled a “divisive concept” during his first administration.
A December 2024 notice in the Federal Register soliciting nominations for committee members said that the panel would, “focus on health disparities in underserved communities … such as but not limited to Black, Latino, and Indigenous and Native American persons, Asian Americans and Pacific Islanders and other persons of color; members of religious minorities; lesbian, gay, bisexual, transgender, and queer persons; persons with disabilities; persons who live in rural areas; and persons otherwise adversely affected by persistent poverty or inequality.”
Health disparities in underserved communities are well documented, as are disparities in accessing medical care.
Research shows that Type 2 diabetes, a condition that often worsens with age and requires frequent doctor’s visits, impacts Black and Latinx Americans at higher rates than White Americans. Rates are also higher in rural areas, with Alabama, Kentucky, Georgia and West Virginia reporting some of the highest. An April 2024 CMS report showed that Indigenous and Black Americans in particular faced barriers to accessing care for diabetes and related conditions.
In the first month of his second presidency, Trump has focused on reducing the size of the federal government and dismantling diversity, equity and inclusion (DEI) and accessibility (DEIA) efforts within federal agencies. Civil rights groups on Wednesday sued the Trump administration over a series of DEI-related executive orders, arguing they were unconstitutional because Trump both exceeded his presidential authority and because the orders discriminated against Black and transgender Americans.
Researchers have warned that the DEI orders are so broad that they could hamper efforts to study race- and gender-identity-related disparities across a variety of subjects, including health care.
A list of diversity-related words that are allegedly banned from being used by federal agencies has been circulating in Washington. Reuters reported Thursday that some scientists at the Food and Drug Administration (FDA) had been told to stop using the words “woman,” “disabled” and “elderly” in external communications. The White House told the newswire that the agency had misinterpreted Trump’s executive orders.
Trump said in an interview with Fox News this week that “Medicare, Medicaid, none of that stuff is going to be touched.” Hours later, he endorsed a GOP budget proposal in the House of Representatives that would gut Medicaid funding. A White House spokesperson told Politico that “the Trump administration is committed to protecting Medicare and Medicaid while slashing the waste, fraud, and abuse within those programs.”
President-elect Donald Trump on Tuesday announced his intent to nominate Dr. Mehmet Oz as administrator of the Centers for Medicare and Medicaid Services. In this photo, Oz speaks at a March 15, 2022 press conference in Harrisburg, Pennsylvania. (Photo by Pennsylvania Capital-Star).
WASHINGTON — Former TV personality and onetime U.S. Senate candidate Mehmet Oz could become the next administrator for the Centers for Medicare and Medicaid Services, an expansive government agency that is responsible for large swaths of the country’s health care.
President-elect Donald Trump announced his intent to nominate Oz on Tuesday, writing in a statement “there may be no Physician more qualified and capable than Dr. Oz to Make America Healthy Again.”
Oz won the Republican primary in the 2022 Pennsylvania U.S. Senate race but was defeated during the general election by Democratic Sen. John Fetterman.
Trump wrote that Oz would “work closely” with Robert F. Kennedy Jr., who will be nominated for Health and Human Services secretary, “to take on the illness industrial complex, and all the horrible chronic diseases left in its wake.”
“He will also cut waste and fraud within our Country’s most expensive Government Agency, which is a third of our Nation’s Healthcare spend, and a quarter of our entire National Budget,” Trump wrote in the announcement.
The Center for Medicare and Medicaid Services manages the country’s largest health care programs, including Medicare, Medicaid, the Children’s Health Insurance Program, or CHIP, and the health insurance marketplaces created by the Affordable Care Act, or Obamacare.
There are 67.7 million people enrolled in Medicare, with nearly 90% of those enrollees over the age of 65. The program also provides health care coverage for younger people with severe illnesses or disabilities.
Medicaid, a state-federal program that provides health coverage for low-income people, has about 72.4 million enrollees.
There are 7.1 million CHIP program participants.
And 21.3 million people purchased health insurance through the ACA marketplace during the 2024 open enrollment period.
When added together, the Center for Medicare and Medicaid Services provides health care coverage to 1 in 4 Americans, according to its latest financial report.
The agency spent about $1.516 trillion during the last fiscal year and has more than 6,700 federal employees as well as contractors to handle the workload.
“CMS and its contractors process over one billion Medicare claims annually, monitor quality of care, provide the states with matching funds for Medicaid benefits, and develop policies and procedures designed to give the best possible service to beneficiaries,” according to the report.
“CMS also assures the safety and quality of medical facilities, provides
health insurance protection to workers changing jobs, and maintains
the largest collection of healthcare data in the United States.”
Oz received his undergraduate degree from Harvard University before earning a joint M.D. and MBA from the University of Pennsylvania School of Medicine and Wharton Business School.
He starred in the daytime show “Dr. Oz,” which ran from 2009 until 2022.
Oz’s nomination is subject to Senate confirmation and is under the jurisdiction of the Finance Committee, currently led by Oregon Democratic Sen. Ron Wyden and Idaho Republican Sen. Mike Crapo.
Oz’s confirmation hearing won’t be the first time he’s testified before a Senate committee. More than 10 years ago, he testified in front of a Senate panel that his comments on his TV show about certain weight loss supplements were “flowery.”
Last updated 5:50 p.m., Nov. 19, 2024
Jennifer Shutt
Jennifer covers the nation’s capital as a senior reporter for States Newsroom. Her coverage areas include congressional policy, politics and legal challenges with a focus on health care, unemployment, housing and aid to families.
Ohio Capital Journal is part of States Newsroom, the nation’s largest state-focused nonprofit news organization.
Ohio Governor Mike DeWine and Lt. Governor Jon Husted today provided the following updates on Ohio’s response to the COVID-19 pandemic.
NURSING HOME VISITATION
Governor DeWine today discussed the new federal regulations for nursing home visitation, as well as Ohio’s Vaccine Maintenance Program. The visitation guidelines, issued by the Centers for Medicare and Medicaid Services (CMS) indicate visitation should be happening in nursing homes. There are a few specific exceptions that would limit visitation, such as outbreaks in the facility or an extreme number of cases in the community. Full information on the federal nursing home visitation guidance is available at cms.gov.
Additionally, Governor DeWine highlighted the progress being made by Ohio’s Vaccine Maintenance Program for nursing homes and assisted living facilities. Ohio’s Vaccine Maintenance Program ensures new nursing home residents and employees, and established residents and employees who previously decided not to receive a vaccine, can still choose to receive one. Governor DeWine emphasized the importance of every nursing home resident receiving a vaccine.
Long-term care facility visitation status is available on the dashboard at coronavirus.ohio.gov.
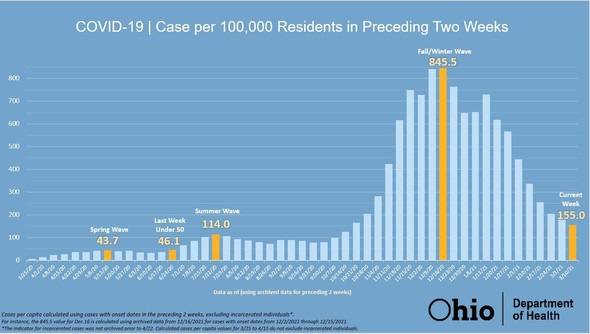
STATEWIDE CASE RATE
Governor DeWine announced that, statewide, Ohio is currently at a rate of 155 cases of COVID-19 per 100,000 people during the past two weeks. Last week, statewide data put Ohio at 180 cases per 100,000 people.
“In Ohio, we are still at a very elevated level of cases, but today’s health data is certainly trending in the right direction,” said Governor DeWine.
In an evening address last week, Governor DeWine announced that when Ohio reached 50 cases per 100,000 people for two weeks, all health orders will be lifted.
The Ohio Department of Health will update this data each Thursday.
RAPID TESTING
Governor DeWine today detailed four initiatives that are making rapid COVID-19 tests more accessible to Ohioans:
Federal Qualified Health Centers
The state’s ongoing partnership with federally qualified health centers has led to the availability of over 150,000 rapid tests at community health centers. These centers have professionals on-hand to administer the tests free of charge.
Local Health Departments
Local health departments have partnered with their communities to make at-home testing available to schools, nonprofit organizations, and first responders.
Public Libraries
The state has recently partnered with public libraries to make at-home tests available to more Ohio communities. During the first two weeks, Ohio has partnering with 120 libraries.
K-12 Schools
A new partnership launched today will bring 200,000 at-home tests to Educational Service Centers. To increase confidence and safety in schools, Governor DeWine encourages school districts to take advantage of this resource and develop aggressive testing plans.
Between libraries and local health departments, at-home testing is accessible in 76 of Ohio’s 88 counties. Some of these areas had disproportionate access to testing earlier in the COVID-19 pandemic.
GUIDANCE ON FAIRS
Governor DeWine announced that the Ohio Department of Health issued a revised order that allows for the reopening of all fair activities if certain health conditions are met. The updated order includes compliance with the statewide mask order and social distancing. Additionally, there will be a 25 percent maximum for indoor grandstand capacity and a 30 percent maximum for outdoor grandstand capacity.
Additionally, the Ohio Department of Health will issue updated order and guidance regarding festivals, parades, proms, and spring sports. For spring sports, students will not be required to quarantine because they have an incidental exposure to COVID-19 in a classroom unless symptoms develop.
These orders and guidance will be forthcoming from the Ohio Department of Health.
LETTER ADDRESSING PUA FRAUD
Governor DeWine and Lt. Governor today sent a letter to President Joe Biden urging the development of a national, coordinated response to ongoing, widespread fraud attempts being committed through the unemployment system, specifically the federal Pandemic Unemployment Assistance (PUA) Program.
See below for an excerpt from the letter:
“We urge you to immediately develop a national, coordinated response to this ongoing attempt to defraud the American people and our national and state governments. While states are doing everything they can to administer the federal programs while maintaining system integrity, a state-by-stare response is proving inadequate. This is not an Ohio problem — it’s a national problem that requires a national solution.”
CURRENT CASE DATA
In total, there are 984,934 confirmed and probable cases of COVID-19 reported in Ohio and 17,825 COVID-19 deaths. A total of 51,323 people have been hospitalized throughout the pandemic, including 7,255 admissions to intensive care units. In-depth data can be accessed by visiting coronavirus.ohio.gov.
Video of today’s full update, including versions with foreign language translation, can be viewed on the Ohio Channel’s YouTube page.
For more information on Ohio’s response to COVID-19, visit coronavirus.ohio.gov or call 1-833-4-ASK-ODH.
Governor Mike DeWine today issued the following statement on nursing home visitation:
The number of new COVID-19 cases in Ohio’s nursing homes has dropped significantly to 343 new cases last week compared to the peak of 2,832 new cases in December.
As the number of nursing-home cases continues to drop due to vaccinations in long-term facilities, Governor DeWine today reminded nursing home staff and families of nursing home residents about the status of visitation in Ohio’s nursing homes. Visitation is permitted at nursing homes in Ohio if the facilities meet the federal Centers for Medicare and Medicaid Services (CMS) criteria to allow visits:
No new onset of COVID-19 cases in the last 14 days;
The facility is not currently conducting outbreak testing; and
CMS reports the COVID-19 county positivity rate at less than 10 percent.
Compassionate care visits, which are special visits in which a family member or other visitor provides comfort, support, and assistance to a resident whose well-being is suffering or at risk, are always permitted regardless of the criteria above.
Governor DeWine sent a letter today to all nursing homes in Ohio reminding them to check their county positivity rate every week to determine their visitation status and to remind them to allow for compassionate care visits.
If you have a loved one in need of a compassionate care visit but are having trouble scheduling a visit, contact Ohio’s Office of the State Long-Term Care Ombudsman at OhioOmbudsman@age.ohio.gov or 1-800-282-1206.
This article provided to Loveland Magazine was edited by David Miller and is by by Eye on Ohio, the nonprofit, nonpartisan Ohio Center for Journalism. Please join their free mailing list as this helps us provide more public service reporting.
In early March, just as Ohioans were learning about the first cases of novel coronavirus in the state, Anna Bondar’s grandfather fell at his Cleveland home.
Luckily, the 92-year old, who lives with dementia, wasn’t injured badly.
The tight-knit family started to discuss the possibility of a nursing home, though they had serious reservations.
Their tough choice was made even more difficult by mounting fears about the coronavirus. In nearly four months, COVID-19 has infected more than 31,191 people statewide and has proven particularly deadly for residents of long-term care facilities in Ohio.
Seventy percent of the reported deaths in Ohio due to COVID-19 complications have been in long-term care facilities, which is among the highest in the country.
Nationally the portion of COVID-19-related deaths in long-term care facilities has hovered just over 40%, though the amount of testing done in nursing homes varies significantly by state.
Every day, families like Bondar’s are making what can feel like an impossible choice – whether to send a loved one to a nursing home where they will receive around-the-clock specialized care but face a greater risk of contracting COVID-19, or to care for that person at home where risk of transmission is lower but providing care can be more challenging.
Even before the pandemic, sorting through the myriad of quality ratings and measures was daunting enough. Then, COVID-19 deaths started to soar.
Now, families and seniors agonize over what could be life or death choice using confusing numbers on infection “hotspots” and without the ability to visit nursing homes to observe how the staff cares for residents – which is the number one recommendation of most advocates.
Dr. Amy Acton, director of the Department of Health
State officials, including Dr. Amy Acton, the former director of the Department of Health, have emphasized that “congregate” settings like nursing homes are at highest risk of infection. Staff, who often travel between facilities, need to be in close contact with residents to provide care. And residents, who are primarily older and have multiple medical conditions, are more susceptible to COVID-19-related complications.
“All of this makes it high risk. At the same time, it’s really necessary for many patients to be there,” said Dr. Steven Schwartz, a geriatric physician at the Cleveland Clinic who travels to nursing homes as part of the Clinic’s Center for Connected Care.
Ohio National Guardmembers will begin testing all staff members and any residents who likely were exposed to COVID-19 in the state’s nursing homes, Gov. Mike DeWine announced May 27. What are being called Congregate Care Unified Response Teams will focus on facilities where confirmed or assumed positive cases are reported in hopes of reducing the number of COVID-19 cases and deaths in Ohio’s nursing homes, which as of May 27 was 5,324 resident cases and more than 1,442 deaths.
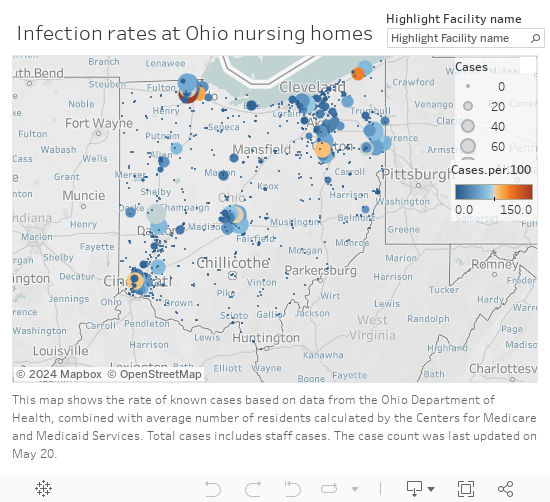
Infection rates in Ohio Nursing Homes
Making an educated decision
Last month, state officials began to release the numbers of reported infections and deaths in long-term care facilities, which include nursing homes, rehabilitation centers, and assisted living centers.
But it’s unclear how much the numbers – which are reported weekly and are also tracked cumulatively – matter for families currently trying to choose a facility.
The state, on its coronavirus website, says the infection and death numbers shouldn’t replace a thoughtful conversation with a nursing facility about infection control practices and that “residents and family members should understand that the presence of COVID-19 at a facility is [in] no way an indicator of a facility that isn’t following proper procedures.”
Yet many in the health care industry say infection information should be considered, along with other factors, when deciding which site to choose.
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck.”
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck,” said Dr. James Campbell, department chair of geriatric medicine at MetroHealth.
The infection information provided by the state can be useful, for instance, if a family is choosing between two similar facilities, said Nate Cyrill, a Long Term Care Ombudsman for Cuyahoga, Geauga, Lake, Lorain and Medina counties.
Since information on the virus changes rapidly, most families still rely on the quality measures that were available before COVID-19, including existing state and federal online guides Cyril said.
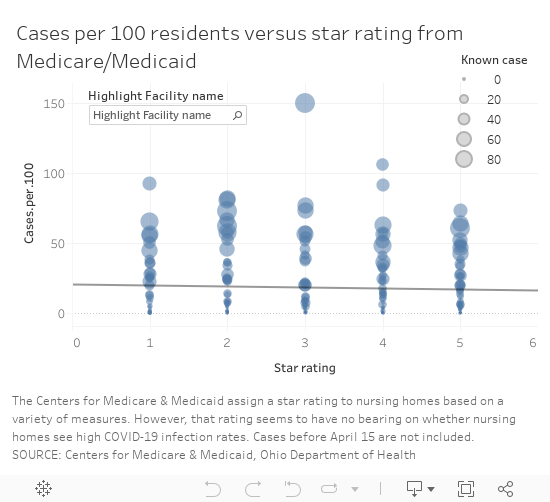
One of the commonly-used ranking systems, maintained by the Centers for Medicare and Medicaid Services, assigns ratings – from 1 to 5 “stars” – to facilities based on performance on quality measures, staffing and inspections.
The number of “stars” Ohio’s nursing homes received, however, does not appear to have a correlation to the number of infections reported to the state, based on a comparison of the publicly available information. The analysis did not include assisted living facilities.
Cases vs. Star rating
“You want to look for a nursing home that’s four of five stars preferably but even that doesn’t tell you the whole story,” Steven Schwartz said.
There are numerous 1-star rated facilities that have reported few infections, like Whetstone Gardens and Care Center in Columbus, which has reported 9 cases or 8 per 100 residents.
Salem North Healthcare Center
Salem North Healthcare Center in northern Columbiana County had 51 patients test positive for the virus as of May 20, as well as five staff, according to the state. It is rated a 5-star facility, the highest rating from CMS.
It’s one of four 5-star facilities with an infection rate over 50 casesper 100 residents, based on Medicare’s calculation of each facility’s average number of residents. (The rate does not include infections among staff because the number of staff in each facility was not available.)
Since April, the focus on high numbers of reported infections, often referred to as clusters, in long-term care facilities has intensified. In some cases, those numbers are a reflection of the level of testing, said Fred Stratmann, general counsel and chief compliance officer for CommuniCare Health Services. It doesn’t mean all of the residents with a positive test had symptoms of COVID-19. The state infection numbers also don’t show the residents who have recovered from the virus, he said.
CommuniCare, which operates close to 90 health care facilities in seven states has been proactive about testing, Stratmann said. When COVID-19 cases started to appear at the North Salem facility, the company enlisted the state’s “strike team” to proactively test all of the residents. It has since re-tested all of the residents who were initially negative and purchased 3,000 testing kits to supplement what the state could provide.
“We wanted to be certain of the extent of COVID in this center in order to be able to properly treat it and to fight back against it,” Stratmann said. The facility does that by isolating any COVID-19-postive patients in a separate unit with its own dedicated staff and by admitting new residents to an observation unit for 14 days to make sure they have no symptoms of infection, he said.
Restrictions on visits make choices harder
The most effective way to scout out a facility typically is to visit it, preferably unannounced, said Dr. James Campbell, department chair of geriatric medicine at MetroHealth. However, because visitors aren’t permitted in nursing homes right now, the next best thing is to ask detailed questions about care, any COVID-19 cases and infection control measures, he said.
Campbell also suggested turning to hospital staff, who work with nursing homes regularly, for advice. Social workers can place five people in a week, while most individuals face that decision, at most, only a few times in their lives, he said.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
The agency, along with other similar independent agencies across the state, investigates complaints in long-term care, skilled nursing, group homes and rehabilitation facilities and can share what are called “verified complaints” that aren’t otherwise available publicly.
Most of the complaints investigated in relation to COVID-19, Cyrill said, have been related to visitation or the ability of families to get information on a loved one’s condition.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
Under normal circumstances, an ombudsperson would go to the facility and talk to patients and could do so without announcing the visit in advance. Since visits are restricted for infection control reasons, they have to work through staff to speak to residents or to ask questions, which isn’t optimal. And they aren’t able to make direct observations.
“It makes our job much more challenging,” Cyrill said.
At the North Salem facility, which has had about a dozen new residents admitted or transfered from other facilities, the staff has given “virtual tours” over the phone to family members or prospective residents who were in the hospital, Stratmann said. The company also invested in technology that won’t replace face-to-face visits but enables more family contact and the ability and for staff to help keep residents’ spirits up by making videos of activities, like dancing and singing, to keep them connected with the local community.
In addition, Stratmann said they walk families through the infection control procedures and share techniques they have implemented to improve health outcomes for patients with COVID-19 including, when appropriate:
Treating residents with anticoagulant medications to reduce the risk of blood clots and strokes, which has been a factor in some COVID-19-related fatalities.
Practicing “proning” or positioning residents, while awake, flat on their belly and chest to reduce the buildup of fluid in lung tissue and reduce the risk of Acute Respiratory Distress Syndrome, which has been associated with many COVID-19 fatalities.
The idea of putting their beloved grandfather in a nursing home was gut-wrenching
Choosing home
For Bondar’s family, the idea of putting their beloved grandfather in a nursing home was gut-wrenching, especially as visitation was curtailed to limit the virus’ spread. He speaks Russian, his native language, and would not have been able to communicate well with the staff caring for him.
“It felt like admitting him [to a facility] would be like saying goodbye,” Bondar said. “Like leaving him to die.”
Bondar’s family ultimately decided to care for her grandfather at home, in his Mayfield Heights senior highrise, where they could limit his exposure to the virus.
Before his fall, an aide visited for about eight hours a week. After the Ohio’s “stay at home” order was put in place March 23, Bondar and her mother were able to work from home and pitch in with care.
The advice of the Clinic’s Steven Schwartz led them to a hospice program, which helped the family find additional aides, including one who speaks Russian, as well as a hospital bed for safer sleeping and a wheelchair.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
“We’ll do this as long as we can manage it,” Bondar said.
Anecdotally, it is a choice more families are making: the decision to use home care or even pull family members out of nursing homes out of fear or because they miss them and can’t visit, Steven Schwartz said.
“Sometimes it’s appropriate. But sometimes, even given everything, it may be safer to have your family member there to get stronger and get the necessary care,” said Steven Schwartz. “I would really try to balance the benefit of going to a nursing home versus the risk.”
Patients with dementia or Alzehimer’s may be unsafe going back home.
Patients with dementia or Alzehimer’s may be unsafe going back home, he said, and families may need to decide if a nursing home really is the safer place.
One of the first orders Ohio put in place to prevent the spread of COVID-19 was to halt in-person visitation in more than 900 nursing and long-term care facilities. The state is not yet ready to lift those restrictions and resume visits in those settings, Gov. Mike DeWine said, but on June 8 will start allowing outdoor visits at assisted living facilities care centers for individuals with disabilities.
“We are not to nursing homes yet and I know that causes anguish for a lot of people who are watching this but we’re trying to do this so that we don’t increase the COVID inside the nursing homes or the assisted living or the immediate care facilities,” DeWine said during a May 28 briefing.
Decisions made harder
Figuring out what kind of care might be best for a patient has become more challenging, too.
Previously, nurses and social workers would visit clients in their homes to assess how they functioned – whether they could independently bathe, cook and grocery shop, said Theresa Foster, a nurse and licensed social worker at Western Reserve Area Office on Aging.
They relied on conversations with clients and family and also observations of the environment in the home and possible risks, said Foster, who runs the agency’s resource center.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Now, those assessments are done by phone and can be done successfully, but it is more difficult, Foster said.
At UH’s hospitals, medical staff use a scoring system to determine the best place for a patient being discharged, said Dr. Sean Cannone, UH’s medical director for population health.
Patients are assessed on their ability to perform daily tasks and on their cognitive abilities.
“We’re trying as much as we can to get patients home if at all possible,” he said. The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
“We want to respond to what people really want for their own care,” Cannone said.
The shift started before COVID-19 cases surfaced but has accelerated as more families worry about potential exposure to the virus in congregate living situations.
As technology has advanced, the capabilities of what can be done in a patient’s home has also increased. In March, UH introduced a new patient management system, Massimo SafetyNet, for remote monitoring.
When patients are released from the emergency room or from a COVID-19 floor, providers now put a bluetooth sensor on their wrist — it looks like an Apple Watch — that streams data about a patient’s vitals to a central monitoring center, said Jonathan Sague, UH’s vice president of clinical operations. That way, providers can make sure a patient is safe at home.
Douglas Beach is the chief executive officer at Western Reserve Area Office on Aging
Douglas Beach, chief executive officer at Western Reserve Area Office on Aging, has had firsthand experience weighing care decisions amid COVID-19 worries. His mother is rehabilitating in a nursing home after a six-week hospital stay related to a heart condition.
Not being able to visit her in the hospital or the facility has been hard, Beach said. He and his brother, who is a doctor, had to make all of the arrangements by phone, including figuring the best way to transport her that would have the lowest risk of exposure to the virus.
“Home and community-based services is what I do,” Beach said. Part of his mission is to advocate for the setting that allows for any person, whether they are older adults or live with a disability, to be as independent as possible .
But for his mother, a nursing facility was the right choice because she needed 24-hour care that her family could not provide at home.
Beach said nursing homes have had to deal with an unprecedented set of circumstances: a new virus, initial unknowns about transmission and populations at extremely high risk for complications.
Nursing homes will continue to play a vital role and will remain the best option for people who need more care than can be safely provided at home, Beach said.
For the more than 9,500 clients his agency serves in Cuyahoga, Geauga, Lake, Lorain and Medina counties, delivering care at home, with health aides, nurses and community and family supports, has proven a low risk. As of mid-May only 35 clients had tested positive for the virus, he said. That is roughly 0.3% of clients, though not all clients are tested.
Managing COVID-19
Cuyahoga County nursing homes have been paired with one of the area’s three largest hospital systems during the pandemic, Campbell said. The hospitals help the facilities both prepare for and respond to COVID-19 cases.
“The goal is when you have one patient in a nursing home with COVID is to make sure you don’t end up with 30 patients with COVID,” Campbell said.
UH developed what is being called a playbook for local nursing homes. The playbook gives facilities a plan for how to respond if there’s a COVID-19 outbreak on-site, said Sague, who works as a firefighter and medic on the weekends.
“It can be pretty startling and pretty alarming if they’re not ready for it,” Sague said.
The playbook gives guidelines on screening, triaging, determining exposure, testing and isolating those who test positive, as well as how to get personal protective equipment, increase staffing and to eventually reopen safely, Sague said.
Once a case is identified at a facility, what is known as an intercept team is dispatched — either virtually or in person — to help a nursing home handle it, he said.
Patrick Schwartz, director of strategic communications for LeadingAge Ohio, a long-term care trade association, said access to testing and safety equipment has been a consistent problem for Ohio’s nursing homes.
But in the past month or so, the state has made “a definite shift” and started prioritizing testing at nursing homes, which is helping, he said.
Patrick Schwartz said he hoped the expanded testing would enable facilities to test their entire population— of residents and staff — so they can better limit the spread of the virus.
Throughout Ohio, populations that have received mass testing — health care workers, first responders, those incarcerated and those in nursing homes — have had higher numbers of positive cases. Many people with COVID-19 are asymptomatic, so it is unknown if they have the virus until they are tested.
“Since this pandemic first reared its head, it was clear to long-term care providers that the front lines would be in long-term care,” Patrick Schwartz said. The populations at those congregate living facilities, many of whom are older and have multiple medical conditions, are among the most vulnerable for complications from COVID-19, he said.
In Cuyahoga County, and elsewhere, local health departments have deployed limited testing resources to nursing homes quickly in hopes of limiting spread in and between facilities and given guidance to homes about how to isolate patients and trace exposures between facilities to limit the spread of infection.
Cuyahoga County Health Commissioner Terry Allan said nursing homes try to guard against outbreaks but have varying degrees of resources. The assistance from the National Guard will allow more residents and staff at facilities in Northeast Ohio to be tested, he said.
Support for this project was provided by the Center for Community Solutions.
Questions to ask:
How can family members stay in touch with residents while visiting is restricted?
Does staff facilitate video visits? Is window visiting allowed?
How often will the facility provide updates on a resident’s condition?
How much COVID-19 testing is being done? Is the facility proactively testing patients or only those with symptoms?
Are private rooms available?
Do staffing ratios allow for residents to be taken outside?
Are residents currently restricted to rooms?
Are separate units and staffs used for COVID-19-positive patients and COVID-19-negative patients?
How does the facility work to limit COVID-19 complications?
Proposed Rule Falls Short of Necessary Measures to Protect Seniors from Unexpected Bills after Colonoscopies
WASHINGTON, D.C. – Today, Senator Sherrod Brown (D-OH) urged the Centers for Medicare and Medicaid Services (CMS) to take the necessary steps to protect seniors from unexpected, out-of-pocket costs following preventive colonoscopies as the Agency considers its annual rule changes. Currently, Medicare charges seniors a twenty percent
Private insurers cannot impose cost-sharing for a screening that leads to polyp removal, but Medicare can charge fees if a polyp is removed.
coinsurance for colonoscopies when a polyp is removed during the procedure even though colorectal cancer screenings are promoted as a free service under Medicare. In December 2018, Brown led 51 of his Senate colleagues in writing to CMS, urging the Agency to act to protect older Americans from out-of-pocket costs for preventive colonoscopies as part of the 2019 updates to the Medicare program.
Each year, CMS makes updates to the Medicare program through notice and comment rulemaking, in which CMS proposes updates to the program, solicits comments from stakeholders, and then finalizes policy changes in a final rule to take effect the following year. CMS released its proposed updates to the program earlier this week, part of which relates to colorectal cancer screenings. In its proposed rule, CMS agreed with Brown’s assertion that these unexpected out-of-pocket costs after a preventive colonoscopy can be “surprise bills” for beneficiaries and solicited comment on ways to improve notice for beneficiaries. However, the proposed rule fell short of taking the necessary steps to protect seniors from these costs. Today, Brown again urged the agency to address this issue in its final rule.
“The most effective preventive action against colorectal cancer is a screening colonoscopy,”Brown said. “Unfortunately, many seniors choose not to undergo this lifesaving procedure because they don’t know if the procedure will be covered by their insurance. I’m urging CMS to update their final rule and ensure all Medicare beneficiaries are protected from unexpected bills after these screenings.”
Brown has also introduced bipartisan legislation to protect seniors from these unexpected costs. In March, Brown, along with Sens. Roger Wicker (R-MS), Ben Cardin (D-MD), and Susan Collins (R-ME), reintroduced bipartisan legislation to protect seniors from out-of-pocket costs for preventive colonoscopies. The Removing Barriers to Colorectal Cancer Screening Act make a long-overdue fix to Medicare to ensure seniors aren’t charged for a colonoscopy – regardless of whether or not a polyp or tissue is removed. Removing harmful tissue during these procedures is key to preventing cancer, yet the fear of having to pay unexpectedly could prevent Medicare recipients from getting these important screenings.
Colonoscopies allow for the detection and removal of polyps that could become cancerous, as well as for the early detection of colorectal cancer when treatment can be most effective. Under current law, seniors covered by Medicare are eligible for colorectal cancer screenings without out-of-pocket costs. However, if a physician takes a further preventive action – like removing a polyp – during the screening while the patient is under anesthesia, the patient is billed as if the procedure was treatment rather than prevention.
Because there is no way of knowing whether a polyp will be removed during a screening colonoscopy in advance, Medicare beneficiaries do not know whether or not their screening colonoscopy will be fully covered until after the procedure is over. This potential cost could lead to Medicare beneficiaries electing to forgo this important preventive screening, even though colorectal cancer screening is promoted as a service without cost-sharing under Medicare. Private insurers cannot impose cost-sharing for a screening that leads to polyp removal, but Medicare can charge fees if a polyp is removed. The Removing Barriers to Colorectal Cancer Screening Act would correct this discrepancy by waiving cost-sharing under Medicare for preventive colonoscopies, even if a polyp or tissue is removed.
Colorectal cancer is the second leading cause of cancer death in the United States for both men and women combined. However, when caught early, it is curable and can even be prevented.








 Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.