
Outside Pickaway Correctional Institution. (Photo Credit Eye on Ohio)
Ohio’s prisons have incubated two of the four largest COVID outbreaks in the nation
A look at how overcrowding and poor design contributed to two of the worst national outbreaks
This article was provided by Eye on Ohio, the nonprofit, nonpartisan Ohio Center for Journalism. Please join their free mailing list as this helps us provide more public service reporting.
For the first two months after the COVID-19 pandemic hit the U.S., Ohio’s response set an example. Thanks to an early shutdown order, the state’s per-capita deaths from the virus as of late April were less than half of those in neighboring Pennsylvania, a state with similar demographics.
But inside the two states’ prison systems, it was a different story.
By late April , the death rate from COVID-19 in Ohio prisons was 22 per 100,000, a rate more than 4 ½ times the overall Ohio rate and nearly twice the national rate.

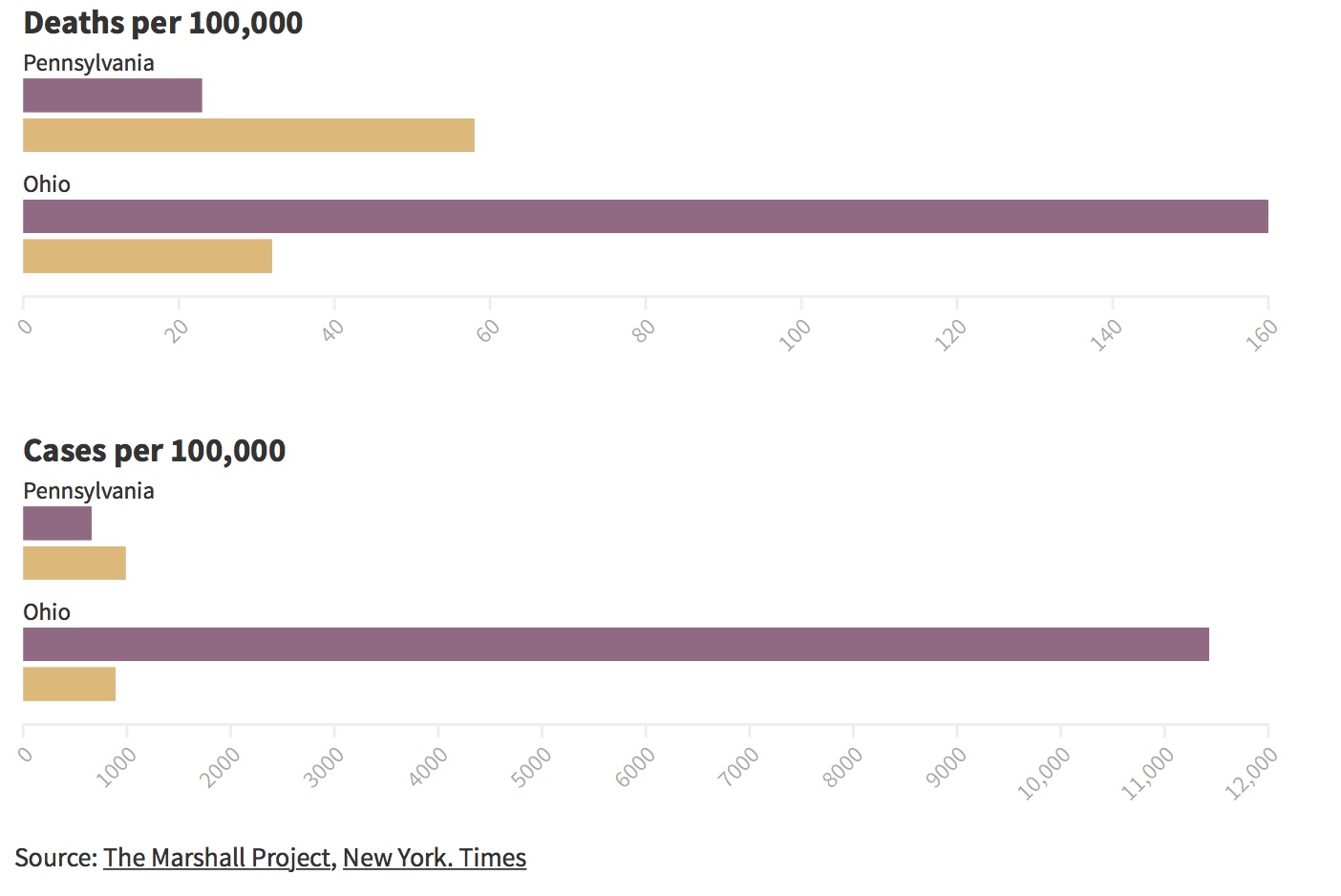
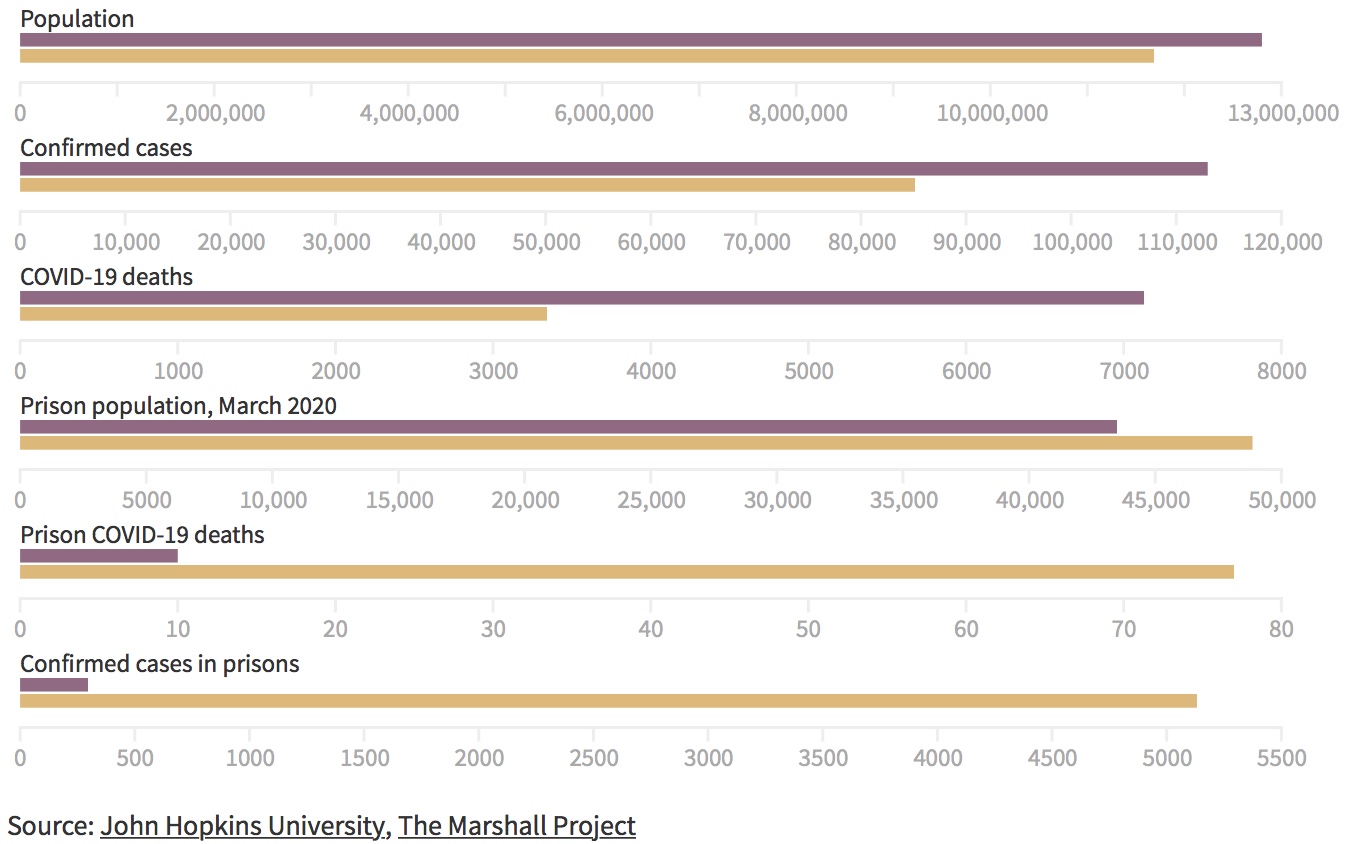
As of August 14, there have been 77 inmate deaths known to be caused by COVID-19, and another 10 suspected— a rate of 160 deaths per 100,000 people. Ohio’s prisons have incubated two of the four largest COVID outbreaks in the nation.
In Pennsylvania’s prison system, which houses about 44,000 inmates at 25 facilities, the death rate was comparatively low— 10 incarcerated people have died as of mid August, for a death rate of 23 per 100,000 people, despite the virus showing up in each state just a few days apart. In fact, a Pennsylvania inmate is less than half as likely to die of COVID-19 as a free Pennsylvanian.
Why have Ohio’s prisons failed so thoroughly to control the spread of COVID-19 when Pennsylvania fared far better?
No state has had a model approach for controlling the virus in prisons. All have made missteps that put inmates’ and staff members’ lives at risk, according to prisoners and prisoner advocates. Prison outbreaks have also spread into the communities outside their walls. But, whether through foresight or luck, factors in some states have kept the virus from running rampant as it has in Ohio prisons. As the country faces new waves of cases, corrections departments may be able to learn from what helped or harmed some states during the first stage of the pandemic.
While advocates for incarcerated people in Pennsylvania caution against holding that state’s experience as a model for how to respond to the pandemic, they agree that the answer may lie both in how crowded the prisons are, and how inmates are housed.
Crowded prisons spread disease
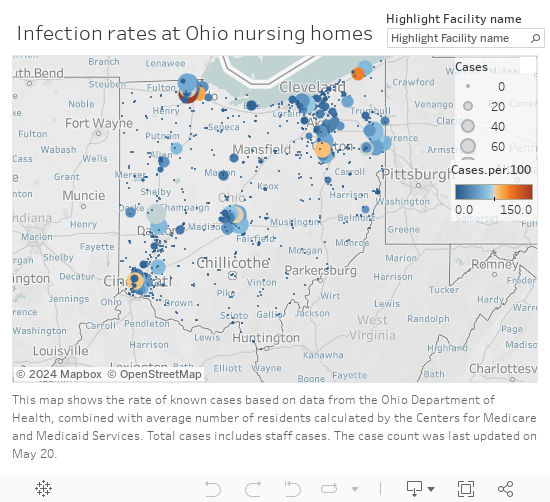
Controlling an outbreak of infectious disease in a prison is never easy. As with other communal living facilities such as nursing homes, once a respiratory illness enters, close quarters gives a virus ample opportunity to spread.
Overcrowding only makes the situation worse.
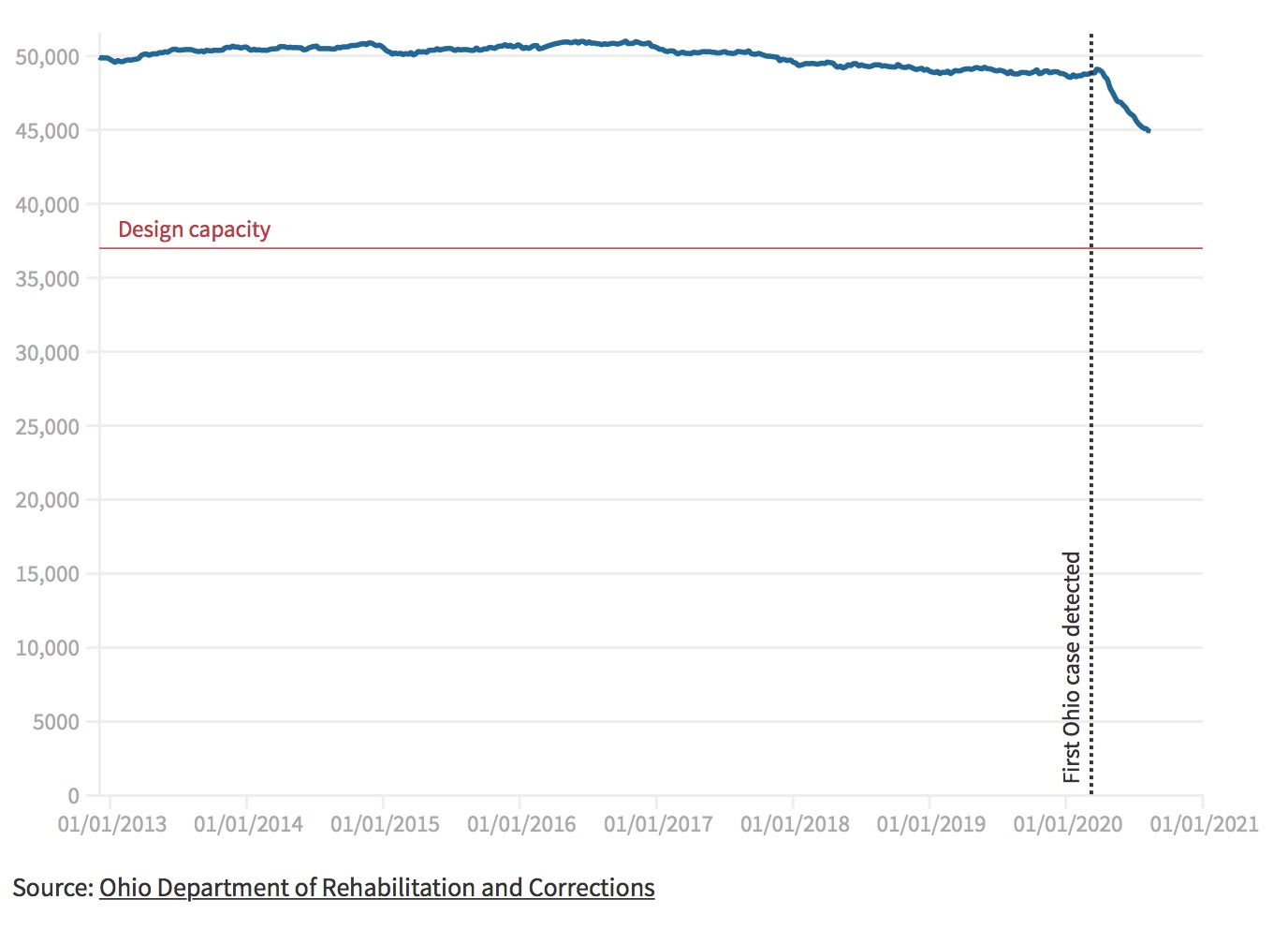
In Ohio, where the prisons were 32% above capacity in February, the virus spread rapidly.
In Pennsylvania’s prisons, at 95% of capacity in February, there were outbreaks in several prisons, but far fewer deaths.
That state’s biggest outbreak to date—183 infections and five deaths among inmates— happened at its oldest prison facility, the 131-year-old State Correctional Institution (SCI) Huntingdon in central Pennsylvania.
“SCI Huntingdon dates from the late 1800’s and has cells with open bars, and four-story housing units with open air shafts to all of the cells,” said Claire Shubik-Richards, executive director of the Pennsylvania Prison Society, a non-profit inmate advocacy organization. “So when the virus came in it spread like wildfire.”
In other, newer Pennsylvania prisons with significant outbreaks, such as SCI Phoenix, the virus proved easier to control. Only 49 inmates at Phoenix, which opened about 2 years ago, have tested positive, and four have died, despite being located in hotspot Montgomery county, just north of Philadelphia.
“The thing about that facility was that the outbreak went up and then went down pretty quickly because it’s a facility where isolating people is pretty easy,” Shubik-Richards said, because it has more single and double-occupancy cells than open dorm units.
In Ohio’s more crowded prison system, the virus was first detected in a staff member in the 66-year-old Marion Correctional Institution on March 29. Less than a month later, nearly 4,000 inmates across the state had tested positive for the virus; 10 were dead, as was one staff member.
Now, the death count is approaching 80. Ohio’s prison system is home to two of the four largest COVID-19 outbreaks in the nation, with 2,440 cases at Marion Correctional Institution in rural central Ohio, and 1,792 at Pickaway Correctional Institution outside Columbus.
Pickaway, built in the 1920s as a mental hospital and converted to a prison in 1984, was designed to hold 1,328 people. As the pandemic began in Mid-March, it held 2,047– 54 percent over capacity.
In one cell phone video that purportedly shows the inside of Pickaway, seemingly endless racks of double-bunked beds are visible, with no barriers and little space between.
“Everybody’s stacked on top of each other, man,” says the person wielding the camera. “Ain’t no social distancing in here….They’re playing with our lives, man.”

Virus runs amok in dorms
Pickaway was designed to have 87% of its beds in open double-bunk dorms, described in a 2015 state prison renovation plan as “barrack-style” (sic), where beds were typically three feet apart. When prisons are overcrowded, staff often squeeze even more beds into the dorms than they were designed to hold, said Meghan Novisky, a Cleveland State University professor who studies how prisons impact health.
In the 2015 master plan, state officials acknowledged that the prison’s dorm-style housing was a problem, not because of disease, but because it elevated prisoners’ stress, setting the stage for unrest.
“A critical need is to improve the dormitory living conditions and reduce the very high levels of crowding,” the report said. “The [Strategic Capital Master Plan] recommends the phased conversion of all dormitory living units to a cubicle-type configuration where inmates will have a higher degree of personal space and privacy.”

Ohio Department of Rehabilitation and Correction (DRC) spokesperson JoEllen Smith said that some of the plan’s recommendations for Pickaway have been implemented. The Orient Correctional Institution, a prison adjoining Pickaway that hasn’t been used since 2001, was demolished, as was Pickaway’s dilapidated E block of dorms. But construction of a new unit with over a thousand beds is on hold due to the pandemic.
Around March 29, leadership at Marion – designed to hold 73% of its inmates in dorms – declared that prisoners in dorms would sleep arranged head-to-foot. That way their faces would be more than three feet apart, according to an email between the prison’s medical services director and the Marion County public health department, obtained by the Documenting COVID-19project at The Brown Institute for Media Innovation.
According to daily statistics released from Ohio DRC, on April 21, more than 28,000 of the state’s 48,396 inmates were either “isolated” or “quarantined.” But in overcrowded prisons where most inmates lived in dorms, both happened in groups, according to numerous inmates.
Daily coronavirus reports from DRC noted that “isolation” meant keeping infected inmates away from those who weren’t sick, while “quarantine” meant “limiting the movements” of someone who may have been exposed to the virus. Guidance issued by the DRC early in the pandemic said it was preferable to quarantine inmates in the infirmary, but if not enough cells were available, they could be “quarantined” in “an area large enough to hold beds and equipment for a minimum of 50 patients.”
Marion was designed to hold 450 inmates in cells. On April 16, 2,417 inmates there were listed as “in quarantine.”
The close quarters of dorm-style housing is a problem in other Ohio prisons, too, inmates reported.
Javalen Wolfe, an inmate incarcerated in dormitory-style housing at Belmont Correctional Institution in southeastern Ohio, said that every time a flu or a cold enters the prison, there’s no stopping it.
“This is how it works because we live so close together. If one person gets sick, everybody gets sick,” he said. “We are literally two feet, maybe two and a half feet between the next person, and there’s no divider, no wall.”
At least nine Belmont inmates had died of COVID-19 as of Aug. 10. Belmont was designed to have 1,855 beds, over 90% of which would be in dorms. As of March 17, near the beginning of the outbreak in Ohio, 2,719 inmates were crammed into the prison— 146% of the population it was meant to hold.
Of the 77 confirmed COVID-19 deaths in Ohio prisons as of mid-July, 67 of them were in prisons that were designed to hold at least half their inmates in dorms. Of the deaths in prisons made up mostly of cells, 10 were in Franklin Medical Center, a small prison dedicated to caring for the system’s most seriously ill inmates.
The worst Pennsylvania outbreaks were at two prisons where inmates were housed almost exclusively in cells – Huntingdon and Phoenix. But the system overall houses just 19% of its inmates in dorms. Roughly 60% of Ohio’s inmates live in dorms, according to Department of Rehabilitation and Corrections Director Annette Chambers-Smith. Each dorm can hold anywhere from 40 to 300 inmates.
And even Pennsylvania’s worst prison outbreaks paled in comparison to Ohio’s. At Huntingdon, the prison with the most deaths, 359 coronavirus cases were confirmed, out of 1,835 inmates. Phoenix housed 2,825 inmates as of late July, 89 of whom tested positive for COVID-19 at some point.
Since mass testing wasn’t conducted at any of the Pennsylvania prisons, the death toll is probably a more faithful indicator of the spread of the disease. The inmate death rate at Huntingdon was 272 COVID-19 deaths per 100,000 people. At Pickaway, it was 1,709, and at Franklin Medical Center, it was over 2,000.
In an interview with Eye on Ohio, DRC Director Annette Chambers-Smith acknowledged that the open bays make it difficult to control the virus. She said they have attempted to mitigate dorm crowding by spreading inmates out in other areas that aren’t normally used for housing, such as gymnasiums and classrooms.
”They literally installed lavatories and facilities in a building so that it could be used overnight to house people,” she said.
And administrators are experimenting with makeshift barriers between dormitory beds at most of its prisons to reduce transmission.
Reducing overcrowding– release of prisoners
Pennsylvania started the pandemic in a relatively good position in terms of space after years of modest, gradual population reduction. They freed up more space after the pandemic hit by giving 3,500 people sentence reprieves and shutting down the county court system.
Several other states have taken steps to free up space in their prisons since the pandemic began, with 15 reducing their prison populations 10% or more between March and June, according to data from The Marshall Project.
Connecticut has taken the most drastic measures, cutting its inmate population by more than 22%, from 12,364 on March 8, the day the virus was first detected in a Connecticut prison, to 9,604 on August 12. Six inmates have died so far in the Connecticut system, which houses only 12,000 inmates thanks to a decade-long pre-pandemic decarceration effort that reduced the population from about 20,000 in 2008.
Compared to the state’s prison population in March, its per-capita death rate has been less than half that of Ohio’s prisons.
That’s despite the fact that, according to prisoner advocate groups in Connecticut, the state made many of the same missteps as Ohio in their attempts to quarantine and isolate inmates.
Melvin Medina, public policy and advocacy director for the ACLU of Connecticut, said that the CDC has recommended isolating people with laboratory-confirmed COVID-19 together and quarantining close contacts together as a group due to limited space in prisons, but did not indicate how large these groups can or should be.
“Our DOC took that to say that in dorm-style settings if there was one sick person in a dorm of 100 people, that meant that whole block was quarantined together,” he said. “They locked sick and healthy people in together and let the virus run its course. In hindsight, I’m deeply thankful that our death count was really low. We could have had a disaster, and we got very lucky.”
Advocates like Novisky say releasing inmates is the best way to protect them from COVID-19, since any group housing makes it hard to control the spread of disease. Even in places where prison populations have dropped by double-digit percentages, advocates say it’s not enough.
“They need to release those that are medically vulnerable,” based on the CDC’s criteria, not just those who are close to the end of their sentences or incarcerated for non-violent offenses, said Nyssa Taylor, criminal justice policy counsel for the American Civil Liberties Union of Pennsylvania. The state is home to about 4,000 older adults serving life sentences, she said, one of the highest such populations in the country.
“I don’t think we should be politicizing who to release,” she said. “I think it’s really important to look at how to save lives, not just ‘release all the non-violent.”’
Meanwhile, Ohio’s prison population fell by about 5.2% between March and June. By August 11, it had fallen 9%.
“I think part of the problem that they’re running into is we really haven’t taken advantage of options to reduce our population size,” said Novisky.
On April 15, Ohio Gov. Mike DeWine announced he was invoking an overcrowding statute to release some prisoners early. Inmates who were within 90 days of their planned release date could be eligible for early release, but only if they met a list of criteria. That excluded people convicted of most types of violent crime, who had served more than one sentence, who had previously been denied judicial release, or who had committed a serious infraction while in prison.
“It basically eliminated everyone,” Novisky said.
Chambers-Smith said the department has taken multiple steps to reduce the population, including reviewing cases of elderly inmates or those with health conditions that make them especially vulnerable to COVID-19. The list of crimes that disqualify inmates for early release under Ohio’s emergency overcrowding law, she noted, is set by the Ohio legislature. The law would have to be amended to loosen those criteria.
“There are more serious crimes where you wouldn’t want to think about people getting out before they’re ready,” she said. “There’s a balancing act here between keeping the public safe and keeping the people in prisons safe.”
Of the 77 Ohio inmates who have died of COVID-19, 34 — more than half— were in prison for sex offenses. Another 18 had been convicted of murder. The average sentences for rape or murder are more than 20 years. Many of the men killed by the coronavirus had grown old in prison.
But most Ohio inmates are serving time for lesser crimes. Only about 12% of Ohio’s inmates were convicted of murder, and 16% were sex offenders. Meanwhile, 15% of Ohio’s inmates were in prison for drug offenses, with 10% serving time for burglary.
But almost a third of Ohio’s inmates released in 2014 ended up back in prison within three years, according to the most recent recidivism study published by the state. All of those prisoners would have been disqualified by DeWine’s exemptions. And with the prisons packed full of repeat offenders, even low-level ones, it would have been difficult to keep older, more vulnerable inmates serving long sentences for more serious crimes isolated.
A spokesperson clarified that it was a joint decision of the governor’s office and the DRC to disqualify repeat offenders, not a stipulation of the emergency overcrowding law.
The day of his announcement, DeWine said he had found 105 people who were eligible for early release, though he noted that more would be considered as they came within 90 days of the end of their sentence.
Since then, the number of inmates has declined slightly, but more due to court shutdowns meaning fewer people sentenced than the slow trickle of early releases. As of August 11, Ohio’s prison population was still nearly 8,000 people over capacity.
Putting the community at risk
Ohio’s prison pandemics also put those outside of prison walls at risk.
As prisons were cut off from visitors, it may have created the false impression that diseases that spread in prisons would stay in prisons. But the Marion outbreak demonstrated otherwise. County health officials and residents voiced concerns in emails that both staff and inmates who finished their sentences were capable of spreading the virus across multiple counties.
In one email obtained by the Documenting COVID-19 project, Traci Kinsler, the Marion County health commissioner, noted that the Marion prison was not isolating inmates before releasing them. Marion released at least one inmate who was known to be infected with COVID-19. He moved to Ashland County.
Marion staff members who contracted COVID-19 lived in at least 20 different counties, according to one message. Two were from out of state.
Chambers-Smith said the department initially offered staff members the option of staying at the facility where they worked to avoid infecting their families. When that offer had few takers, they contracted with hotels to give prison workers a place to sleep, or at least shower before they went home.
Inmates are tested before their release dates, she said, and those who were selected for early release have their release dates pushed back if they test positive until they are considered recovered— officially defined by the department as 14 days past the onset of symptoms, and 72 hours symptom-free. If they reach their regularly scheduled release date, the department has no authority to keep them incarcerated, but will release COVID-positive people with a quarantine order. She said the department collaborates with health departments and religious organizations to give them a place to liveand supplies so they can self-isolate.
Kinsler told Eye on Ohio that the Marion prison outbreak flooded the Marion Public Health Department with cases all at once, and at first officials in various departments struggled with contact tracing. They were able to contact most of the infected people who were released, though, and alerted the county health departments where they settled.

Ultimately, most of the 2,532 people known to be connected to the outbreak at Marion Correctional were either inmates or staff. But the virus made its way to an additional 58 people outside the prison, including family members, health care workers and food workers.
And there could be other cases where health workers simply forgot to label the infection as related to the Marion prison outbreak in the database.
Chambers-Smith said the danger works both ways.
”If there’s COVID out in the community, there’s COVID in the prisons,” she said.
This story is sponsored by the Northeast Ohio Solutions Journalism Collaborative, composed of 16-plus Greater Cleveland news outlets including Eye on Ohio, which covers the whole state.



 Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services. 

