In addition to overseas wars and continuing supply-chain disruptions, diseases and climate-driven storms are making it hard to feed the hungriest Ohioans, Ohio’s top food bank official said Friday.
And that’s even as continuing inflation is creating ever more of them, she said.
“We’re just not seeing a return to normal at all,” said Lisa Hamler-Fugitt, executive director of the Ohio Association of Foodbanks.
Throughout the pandemic, Ohio’s food banks have seen record demand. Now, with costs of essentials like food and utilities continuing to increase, things are only getting worse.
“We thought we were at the high-water mark for demand,” Hamler-Fugitt said. “We’re way past that.”
She said that in the quarter ending Sept. 30, Ohio’s overstretched food banks saw 50% more children than they had in the same quarter of an unusually busy 2021. They also saw 31% more seniors, she said.
“Once people start getting these high heating costs, this will continue,” she said. “Seniors are just outliving their resources.”
In addition, Putin’s war in Ukraine continues to keep grain and other agricultural products off the market and while gas prices are coming down, prices for the fuel mostly used to transport food — diesel — remain high. All those factors increase food prices at the same time that food banks are having to buy more because USDA food donations have been cut substantially.
To help with those purchases, Gov. Mike DeWine in October announced that food banks would get $15 million in unexpended federal coronavirus funds — money that Hamler-Fugitt said is going to buy protein-rich food like beef, ham, poultry, eggs and dairy products. Last week, the legislature announced another $25 million for the food banks, which Hamler-Fugitt said would be evenly split between proteins and plant-based foods.
But as the food suppliers of last result scramble to meet demand, mother nature seems to be conspiring against them.
“Most of our vegetable production this time of year shifts to the South and the West Coast,” Hamler-Fugitt said.
In addition, the coronavirus isn’t the only disease increasing food costs. An avian flu outbreak has impacted more than 44 million birds, trebled egg prices and also inflated the cost of Thanksgiving and Christmas turkeys.
All of which adds to the burden shouldered by foodbanks. Hamler-Fugitt acknowledged that she’s been appealing for help since the start of the pandemic and said she understands that covid fatigue set in long ago. But she said the number of hungry Ohioans is still growing.
“We’re just bracing and hoping that something else doesn’t happen,” she said.
This story was originally published by ProPublica. ProPublica is a Pulitzer Prize-winning investigative newsroom. Sign up for ProPublica’s The Big Story newsletter to receive stories like this one in your inbox.
Late one afternoon last October, Dr. Shelley Odronic sat in her office and, just as she had thousands of times before, slid a rectangular glass slide onto her microscope.
A pathologist who works in rural Ohio, Odronic leaned forward to examine tissue from the placenta of a woman who had recently given birth. She increased the magnification on the microscope. Never had she seen so many tiny, congealed reservoirs of blood or such severe inflammation of the tissue, a sign the placenta had been fighting an infection.
“Right away, I knew it wasn’t compatible with life,” Odronic said.
She asked her secretary to print out the patient’s chart. In dark letters were the words “fetal demise.” A stillbirth, the death of a fetus at 20 weeks or more of pregnancy. But that didn’t solve the mystery. Odronic had examined many placentas from pregnancies that ended in stillbirth. None looked like this — withered and scarred.
Odronic kept reading. No chronic medical conditions. Good prenatal care. Then, buried in the middle of the report, she spotted something. Seven days before the stillbirth, the mother had tested positive for COVID-19. Odronic wondered if the virus could explain the damage to the placenta. In the world of placenta pathology, a new affliction is unusual, especially one so dramatic in presentation and so devastating in effect.
In the world of placenta pathology, a new affliction is unusual, especially one so dramatic in presentation and so devastating in effect.
Her mind traveled to Dr. Amy Heerema-McKenney, a pathologist at Cleveland Clinic and an expert on the placenta, who had trained Odronic during residency. Odronic went to sleep that night with a pit in her stomach and a plan to call her former teacher in the morning.
Heerema-McKenney was in her office when the phone rang. As she listened, she knew that what Odronic was describing was what she and her colleagues had observed repeatedly over the past several months: a patient positive for the coronavirus, a placenta destroyed by COVID-19, a baby stillborn.
Their next discovery was equally stunning. None of the stillbirths they studied involved a pregnant person who had been fully vaccinated. The doctors checked with colleagues across the country and around the world. The fatal pattern held.
Unvaccinated women who contracted COVID-19 during pregnancy were at a higher risk of stillbirths. They also were more likely to be admitted to the intensive care unit, give birth prematurely or die. Yet their greatest protection — the COVID-19 vaccine — sat largely untouched, buried under doubt, polluted by disinformation.
Pharmaceutical companies and government officials failed to ensure that pregnant people were included in the early development of the COVID-19 vaccine, a calamitous decision made amid the urgency of a rapidly spreading pandemic. That decision left pregnant people with little research to rely on when making a critical decision on how best to keep the babies growing inside of them safe.
Their greatest protection — the COVID-19 vaccine — sat largely untouched, buried under doubt, polluted by disinformation.
At the same time that research was excluding pregnant people from vaccine trials, a full-scale assault on vaccination was unfolding online. Taking advantage of the lack of data, conspiracy theorists, anti-vaxxers and even some medical professionals spread false claims about the vaccine’s safety in pregnancy, leading many pregnant people to delay or refuse the vaccine. Even now, with numerous studies unequivocally announcing the safety of the vaccine for pregnant people, some doctors have failed to communicate the dangers of COVID-19 to pregnant people or the vaccine’s role in mitigating it.
The Centers for Disease Control and Prevention contributed to the confusion with vague early messaging about whether pregnant people should get vaccinated. While Americans lined up at pharmacies and stalked vaccine websites in hopes of securing a shot last year, pregnant people had some of the lowest vaccination rates among adults, with only 35% fully vaccinated by last November. Meanwhile, many Americans were already moving on to their boosters after federal officials that month expanded eligibility for the additional shots to anyone 18 or older. And much of the country was beginning to return to pre-pandemic life. The Sunday after Thanksgiving, for instance, set the record for the busiest day of air travel since March 2020.
November also marked a key moment in the understanding of COVID-19’s impact on stillbirths. A CDC study looking at 1.2 million births in the first 18 months of the pandemic found that more than 8,000 pregnancies ended in stillbirths, including more than 270 of them in patients with a documented COVID-19 diagnosis at the time of delivery.
Although stillbirths were rare overall, babies were dying. The risk of a stillbirth nearly doubled for those who had COVID-19 during pregnancy compared with those who didn’t. And during the spread of the delta variant, that risk was four times higher.
The risk of a stillbirth nearly doubled for those who had COVID-19 during pregnancy compared with those who didn’t.
Indeed, doctors discovered that some stillbirths resulted from COVID-19 directly infiltrating the placenta, a condition they named SARS-CoV-2 placentitis. Cases were found even in people whose COVID-19 symptoms were mild or nonexistent. In some cases, however, placentas were discarded with medical waste without being tested for COVID-19, and parents never learned what led to their baby’s stillbirth.
COVID-19 also led to stillbirths among pregnant people who became exceedingly ill after contracting the virus. It damaged their lungs and clotted their blood, putting their babies in such severe distress that they were born before they could take their first breath.
“These are pregnancies that should not have ended,” Heerema-McKenney said.
She and others had tried to alert the CDC as well as maternal and state health organizations to their findings, but she said they either didn’t get a response or were told they needed to collect more data and publish studies. Pathologists are experts in disease diagnosis, dealing with death and illness from the safe distance of their labs. Convincing obstetricians who met with patients daily or doctors who were making policy recommendations was a challenge.
“I tried to sound the alarm. We tried so hard to get people to listen,” Heerema-McKenney said. “It was a really frustrating place to be as pathologists doing these autopsies, looking at these placentas and saying, ‘God, no, not another case.’”
Around the same time Heerema-McKenney was examining the damaged placentas, Ginger Munro was on life support in a hospital 250 miles away in another part of Ohio.
She and her husband, Kendal, had been trying to have a child for five years. They hadn’t expected that she’d get pregnant in the middle of a pandemic. But when her pregnancy test came back positive in the spring of 2021, she rushed to post a picture of it in an online pregnancy group. “Is it just me or can you see the 2 lines??” she asked.
The pandemic had already brought much change to their lives. Ginger, who lives in the small town of Washington Court House in southwest Ohio, quit her job as assistant nutrition director with the county’s Commission on Aging. She stationed hand sanitizer throughout her house and in her car, and she only went grocery shopping early in the morning. If she noticed someone in an aisle, she skipped it.
“I knew the virus was real,” she said, “but I was terrified to take the vaccine.”
Ginger worried that the vaccine’s development had been rushed, and she hadn’t seen any data showing it was safe for pregnant people. At this point, the CDC had not explicitly recommended the vaccine during pregnancy. Ginger already worried she was tempting fate by getting pregnant at 40; she said she didn’t want to risk endangering her baby by taking the vaccine.
Besides, if it was really important, her doctor would have mentioned it, and, she said, she would have followed his advice. But, she said, he never did. Her family hadn’t gotten vaccinated either. In a mostly rural county where less than half of the residents were vaccinated, they were hardly alone.
Her doctor declined to comment through a spokesperson at the hospital system where he works; the spokesperson said the hospital couldn’t disseminate information about the vaccine to pregnant patients before it was recommended.
Ginger’s pregnancy progressed without complications. She and Kendal shared the news of a new baby with Ginger’s two daughters from a previous marriage. At their kitchen table, near a sign that read “eat cake for breakfast,” Sophia, then 14, covered her mouth with both hands while Hailee, then 18, simply beamed.
At a backyard gender reveal three months later, Ginger’s growing belly resembled a basketball against her tiny frame. She leaned in to kiss her husband, her long, dark hair falling onto her shoulders. Red confetti rained down on the deck.
Kendal, an aircraft maintenance and avionics manager at an airport two counties away, worked through the pandemic. In the summer, when they realized his cough was actually COVID-19, it was too late. Ginger was sick.
When they realized his cough was actually COVID-19, it was too late. Ginger was sick.
Having trouble reaching her doctor, she went to two different emergency rooms. One, she said, declined to treat her with monoclonal antibodies, which research had shown can be an effective treatment for pregnant people with COVID-19. The other, which described her in medical records as “an exceedingly pleasant individual admitted with symptomatic COVID-19 pneumonia,” transferred her about an hour away to the University of Cincinnati Medical Center. There, records show, she was admitted with acute respiratory distress syndrome due to COVID-19.
The University of Cincinnati doctor asked Ginger and Kendal — who was on FaceTime because of the hospital’s COVID-19 protocols — about “fetal priority.” Ginger made her wishes clear: Save the baby, their baby, the baby they had tried so hard to have. Kendal, who was worried about both his wife and their unborn child, said he went along with Ginger in that moment.
“You were so scared,” Kendal wrote in a notebook that night. “We told each other over and over how much we loved each other.”
They hung up so the doctors could insert a breathing tube. Before they could begin, Kendal called back three more times just to hear her voice.
Doctors put Ginger on ECMO, a form of life support reserved for the sickest patients. Kendal, Hailee, Sophia and Ginger’s mother and sister were later allowed in the hospital two at a time, and they prayed at her bedside nearly every night. Ginger was sedated, her face swollen and obscured by tubing, her cheeks flattened by the crush of the ventilator straps, her wrists tied down so she wouldn’t accidentally pull out her breathing tube.
Her family took solace in knowing the baby’s heartbeat was steady and her ultrasounds were normal. The doctors gave Ginger medication to help the baby’s lungs mature in case she was born early. After more than 30 days on ECMO, doctors took Ginger off the machine only to put her back on the next morning. She was the first patient in the hospital’s history to be placed on ECMO twice.
The plan, records show, was to deliver at 28 weeks. But the day after Ginger was put back on life support, Kendal got the call telling him the baby was on her way. As doctors prepared for the delivery in Ginger’s intensive care room, the family camped out in the waiting room, jittery from excitement and vending machine snacks. They talked about baby names and future family outings. They pulled the waiting room chairs together to form makeshift beds and covered themselves with blankets they brought from home.
They don’t know if they actually fell asleep before a nurse burst through the doors screaming at them to follow. “She’s coming! She’s coming!” They didn’t make it far before they were blocked by doctors and nurses, some huddled over an incubator in the middle of the hall and the rest crowded around Ginger.
Hailee tried to peer over the sea of blue scrubs to catch the first glimpse of her little sister. She smiled beneath her black mask. She’ll be OK, she said to herself.
But after a few minutes of trying to revive the baby, a doctor told Kendal it was time. Kendal nodded, asked for a chair and collapsed as he tried to process his daughter’s death.
Then another wave of grief washed over him. Someone would have to tell Ginger.
Ginger’s medical records describe a baby born at 27 weeks “without signs of life” after an “uncomplicated delivery.” Her placenta had separated from the wall of the uterus, the risk of which studies have shown increases with COVID-19.
When Ginger woke up, she looked down at her sunken belly and realized she had given birth. She assumed her daughter was in the newborn intensive care unit. Ginger was barely able to speak around the tube in her trachea, but after a few days in which no one brought the baby to her, she couldn’t wait any longer. Ginger turned to her mother and sister and mouthed the words, “Where’s the baby?”
When Ginger woke up, she looked down at her sunken belly and realized she had given birth. She assumed her daughter was in the newborn intensive care unit.
The room fell silent. They called Kendal, who rushed to the hospital. He told her what had happened. He described their daughter’s dark hair and her long fingers and toes, just like her mother’s.
Ginger, who had always loved the sweet smell of a newborn’s breath, whispered to her husband.
“Did you smell her breath?”
“She wasn’t breathing,” he said.
In the hurried quest for a safe and effective COVID-19 vaccine, pharmaceutical companies and government officials did not include pregnant people in their initial plans. It’s a failure that continues to reverberate.
“They absolutely should have been included in COVID vaccine trials from the beginning,” said Kathryn Schubert, president and CEO of the Society for Women’s Health Research, a Washington, D.C.-based nonprofit that advocates for the inclusion of women in research and clinical trials.
Researchers and advocates have spent more than four decades trying to dismantle the belief that it’s unsafe or unethical for pregnant women to participate in clinical trials. A couple years ago, it seemed like they had finally prevailed.
Shortly before leaving office, President Barack Obama signed into law the 21st Century Cures Act, which established the Task Force on Research Specific to Pregnant Women and Lactating Women. The group found longstanding obstacles, including liability concerns, to including pregnant and lactating people in clinical research. It concluded that recommending halting medication or forgoing treatment while pregnant may actually endanger the health of the mother and her fetus more than the treatment itself.
The need for everything from asthma to depression medication doesn’t stop when a person gets pregnant, and when a catastrophic event such as a pandemic hits, experts said, pregnancy should not preclude someone from receiving life-saving treatment.
Around the same time, researchers discovered that the Zika virus, which was mainly transmitted through mosquitoes, could pass from a pregnant person to their fetus and cause severe birth deformities. A second group of experts joined together to develop separate guidance on including pregnant people in the research, development and deployment of pandemic vaccines.
Both groups pushed to remove pregnant women from a list of vulnerable populations that required additional review before being allowed to participate in research. Instead of proving that pregnant women should be included, manufacturers would need to provide compelling evidence for why they shouldn’t.
In 2018, the federal task force issued recommendations calling for including pregnant and breastfeeding people in biomedical research, and the Department of Health and Human Services adopted some of the guidance. But a gap remained between what the task force and others insisted was needed and what was actually happening.
“We were frustrated because COVID-19 provided an opportunity to implement the recommendations of the task force,” said Dr. Diana Bianchi, the director of the Eunice Kennedy Shriver National Institute of Child Health and Human Development and the chair of the task force.
In February 2021, Bianchi and her colleagues published an article lamenting the exclusion of those who were pregnant or breastfeeding from the initial COVID-19 vaccine clinical trials. “Pregnant and lactating persons should not be protected from participating in research, but rather should be protected through research,” they wrote.
Ruth Faden, the founder of the Johns Hopkins Berman Institute of Bioethics, helped lead the group that issued the guidance after Zika. She and others urged manufacturers to include pregnant people in the development of the COVID-19 vaccine as part of Operation Warp Speed, the federal program that provided billions of taxpayer dollars to pharmaceutical companies to speed up vaccine production.
“There is a playbook in place so that when the U.S. launches Operation Warp Speed, it should be pretty obvious what should be done,” she said. “It’s not like no one knows how to do this, either ethically or technically.
“Nevertheless, it doesn’t happen,” Faden added. “Once again, pregnant people are left behind.”
A spokesperson for Pfizer said the company followed guidance from the Food and Drug Administration. Although pregnant people were not included in the initial vaccine clinical trials, Pfizer tested its vaccine on pregnant rats and did not identify any safety concerns. The company subsequently launched a clinical trial with pregnant women but halted it because at that point the vaccine had already been recommended for pregnant people.
Similarly, Moderna also studied its vaccine on pregnant animals, but the company said it made the decision “to prioritize the study of the safety and efficacy” of the vaccine in adults who weren’t pregnant. It called that approach “consistent with the precedent to study new vaccines in pregnant women only after demonstration of favorable benefit and risk in healthy adults.”
In response to questions from ProPublica, Johnson & Johnson referred a reporter to its website, which didn’t address the relevant issues.
Some government officials, including several from the Food and Drug Administration, said they support having pregnant women take part in clinical studies of vaccines for emerging infectious disease, including COVID-19. A spokesperson for the National Institute of Allergy and Infectious Diseases, which is part of the National Institutes of Health, said the agency did not “dictate the protocol development” for the trials and said that responsibility lies with the companies.
The failure to include pregnant people early on in COVID-19 vaccine trials was, at least in part, a casualty of the tremendous urgency to respond to an intense public threat and develop the vaccine as quickly as possible, Faden said. But multiple groups had published road maps on how to ethically include pregnant people without slowing down that process.
“I can’t tell you how many pregnant people might not have died or how many stillbirths might not have occurred if the playbook had been followed,” she said, “but I’m willing to bet it was a significant chunk that would have been prevented if there had been a full-throated, evidence-based recommendation for COVID-19 vaccines in pregnancy almost simultaneous to when it was available for the rest of the adult population.”
“I can’t tell you how many pregnant people might not have died or how many stillbirths might not have occurred if the playbook had been followed,” she said.
By the time the CDC specifically recommended the vaccine for pregnant people, in August 2021, the damage had been done.
A dizzying and vague series of advisories led to confusion and delayed vaccinations. When the COVID-19 vaccines were first made available in December 2020, the CDC said health care workers and residents of long-term care facilities should be prioritized, but the shots were not explicitly recommended for pregnant people. Instead, the agency said on its webpage for vaccines and pregnancy that pregnant health care workers “may choose to be vaccinated.” In explaining that decision, the CDC said that experts had considered how mRNA vaccines, which do not contain the live virus, work. They concluded that the vaccines “are unlikely to pose a risk for people who are pregnant.”
“However,” the CDC added, “the potential risks of mRNA vaccines to the pregnant person and her fetus are unknown because these vaccines have not been studied in pregnant women.”
In January, the World Health Organization recommended against pregnant people getting the vaccine unless they faced increased risk, such as complicating comorbidities or exposure to the virus due to a job in health care, but the agency later reversed course.
A few months later, in March 2021, the CDC continued its lukewarm messaging that pregnant people “may choose” to be vaccinated. The agency listed some points for pregnant people to consider discussing with their health care providers, starting with how likely they are to be exposed to COVID-19.
After a promising study showed that the vaccine was safe for pregnant people, CDC Director Dr. Rochelle Walensky said at a White House briefing in late April that the CDC was recommending the vaccine for them. But the CDC did not update its website to reflect her comments and said the agency’s guidance had not changed: Pregnant people “may choose to be vaccinated.”
Once again, pregnant people were put in the precarious position of receiving ambiguous and inconsistent recommendations. In May 2021, the CDC reiterated that pregnant people faced an increased risk of getting severely ill from COVID-19, but the language surrounding the vaccine — “If you are pregnant, you can receive a COVID-19 vaccine” — was noncommittal.
A CDC spokesperson, responding to questions from ProPublica, said in an email that pregnant people were part of the first recommendations in December 2020 that encouraged people 16 and older to get vaccinated. At that time, data about the safety and efficacy of the vaccine during pregnancy was limited “because pregnant people had been excluded from pre-authorization clinical trials,” so the CDC included additional supporting language for pregnant people, saying they were eligible and could choose to receive the vaccine. The agency said its recommendations were based on available evidence and evolved throughout the pandemic.
Before making changes to its guidance, the CDC had its team of scientists review available data to ensure that there was “an abundance of evidence.”
“For each update to the statement of risks during pregnancy, multiple types of studies and the strength of evidence for each were reviewed,” another CDC spokesperson said. “These reviews of the evidence were accompanied with discussions among subject matter experts both internally and externally with clinical partners for an ultimate determination of risk.”
Dr. Cynthia Gyamfi-Bannerman, a perinatologist and chair of the department of obstetrics, gynecology and reproductive sciences at the University of California, San Diego School of Medicine, shared the daunting task of making vaccine recommendations for pregnant people as part of COVID-19 task forces for two leading organizations, The American College of Obstetricians and Gynecologists and the Society for Maternal-Fetal Medicine.
In the beginning, she said, the only pregnancy-specific data they had came from a few dozen participants who were inadvertently included after becoming pregnant during the clinical trials and from some pregnant animal data.
“It played out in real time in the COVID pandemic because we see the effects of not including pregnant people in these trials,” Gyamfi-Bannerman said. “We couldn’t make a strong recommendation, so pregnant people were hesitant. I think that directly led to fewer people using the vaccine than we would have wanted.”
At the end of June 2021, the CDC added a general update to its website to reflect the dangers of the delta variant tearing across much of the country. “Getting vaccinated prevents severe illness, hospitalizations, and death,” it wrote. “Unvaccinated people should get vaccinated and continue masking until they are fully vaccinated.”
But it wasn’t until Aug. 11, eight months after the first vaccine was administered, that the CDC issued its formal recommendation that pregnant and breastfeeding people get vaccinated.
“The vaccines are safe and effective,” Walensky said in a statement at the time, “and it has never been more urgent to increase vaccinations as we face the highly transmissible Delta variant and see severe outcomes from COVID-19 among unvaccinated pregnant people.”
August would prove to be the deadliest month for COVID-19-related deaths of pregnant people. The CDC issued an emergency call the next month strongly recommending the vaccine to pregnant people, noting that approximately 97% of pregnant people hospitalized with COVID-19 were unvaccinated. The dangers to symptomatic pregnant people included a 70% increased risk of death, and their developing babies could face a host of perils, including stillbirths.
August would prove to be the deadliest month for COVID-19-related deaths of pregnant people. The CDC issued an emergency call the next month strongly recommending the vaccine to pregnant people, noting that approximately 97% of pregnant people hospitalized with COVID-19 were unvaccinated. The dangers to symptomatic pregnant people included a 70% increased risk of death, and their developing babies could face a host of perils, including stillbirths.
Researchers have yet to determine exactly why some pregnant people with COVID-19, vaccinated and unvaccinated alike, deliver stillborn babies, while others do not. Attempts to answer that question have been hindered, in part, by incomplete data. The CDC’s statistics on COVID-19-related fetal and maternal deaths are undercounts. The CDC has data on less than 73,000 birth outcomes following a mother’s confirmed COVID-19 diagnosis in 2020 and 2021, of which 579 were pregnancy losses.
That information was sent in by fewer than three dozen health departments, and those estimates don’t include states like Mississippi, which in September reported 72 COVID-19-related stillbirths since the start of the pandemic, nearly double what the state would have expected, according to data from the Mississippi State Department of Health. Preliminary state data shows total stillbirths increased there in 2020 then dipped in 2021, but were still higher than pre-pandemic numbers.
A separate CDC database shows more than 220,000 COVID-19 cases and at least 305 deaths among pregnant people.
“CDC recognizes that pregnant people faced challenging decisions about how to best protect themselves in the setting of uncertainty related to both the infection and the COVID-19 vaccine,” a CDC spokesperson said, adding, “COVID-19 vaccination remains one of the best ways to protect yourself and your family from serious illness from COVID-19.”
Heartbroken and determined, Jaime Butcher has emerged as an unofficial ambassador for the vaccine, posting in online pregnancy and stillbirth forums about the risks of being pregnant and unvaccinated.
No one, she said, told her of the risks. Doctors, the CDC and health officials, she continued, aren’t doing enough to inform people. Even now, well into the pandemic’s third year, the message still isn’t getting through.
No one, she said, told her of the risks. Doctors, the CDC and health officials, she continued, aren’t doing enough to inform people. Even now, well into the pandemic’s third year, the message still isn’t getting through.
“I kept seeing it happening more and more to women and it wasn’t talked about,” she said. “They just say, ‘Oh, get the vaccine,’ which is great, but they don’t talk about what getting the virus can do to pregnant women.”
As a wedding planner, Butcher was surrounded by love. She found it with her husband, then in the daughter growing in her belly, who they named Emily after Butcher’s grandmother.
Butcher suffered five miscarriages before, she said, she opened an email from an in-vitro fertilization clinic confirming her pregnancy in the summer of 2020. She screamed, and her husband rushed to wrap her in a hug.
They waited until she was five months along to announce her pregnancy at Thanksgiving. The next day, Black Friday, they bought a high chair, a tummy time mat and pink onesies.
They were taking precautions, Butcher said, especially since the vaccine wasn’t yet available to her or her husband. But a week later, she woke up with a runny nose, though she didn’t think much of it. Still, she went to the hospital to make sure everything was OK. An ultrasound came back normal.
When her daughter’s kicking slowed the next morning, she called her doctor’s office again. They told her to eat something sweet to get the baby moving. She tried everything she could find: orange juice, Cheerios, Twix, graham crackers, peanut butter and jelly. Nothing worked.
A few hours later, Butcher drove herself to the hospital, where she followed her daughter’s heartbeat on the screen. Steady. Then slow. Then still.
A few hours later, Butcher drove herself to the hospital, where she followed her daughter’s heartbeat on the screen. Steady. Then slow. Then still.
She delivered at 23 weeks. Butcher didn’t know she had COVID-19 until they tested her at the hospital. A lab report later revealed extensive damage to the placenta.
“I was in shock. I was in shock that I lost my daughter, in shock that I had COVID,” Butcher said. “She should be alive, but it’s because of COVID that I lost her.”
A week later, she parked in front of Kohl’s to return the high chair, the clothes still on tiny hangers and the stroller her mom gave her. As she made her way to the register, she saw a baby in an identical stroller. The tears stung all the way down her cheeks.
“You see what you want right in front of you,” she said, “and it’s like, ‘My baby should be here. This shouldn’t have happened.’”
Even before the pandemic, almost a quarter of all stillbirths may have been preventable. The stillbirth crisis has simmered silently in the U.S., claiming the lives of more than 20,000 babies annually. But parents often suffer alone, overwhelmed by grief and guilt.
Butcher, now 45, scheduled her vaccine as soon as she could. Her second dose fell on what was supposed to be Emily’s due date. After getting the shot, she and her husband drove up to Cleveland to visit their daughter’s grave and tell her that her mother got the vaccine in her honor. They let her know how much she was loved and how desperately they wished she was still safe inside her mother’s womb.
They didn’t linger long that spring day. It was a quiet visit. Butcher brought Emily pink flowers, always pink, and said goodbye.
They didn’t know it at the time, but they’d be back in a year to introduce her to her little brother.
Amid the devastation of the pandemic, Heerema-McKenney sees a glimmer of hope. The antibodies from the vaccine have been shown to transfer through the placenta. That immunity in the womb, research shows, reduces the risk of the youngest infants being hospitalized with COVID-19. She continues to encourage pregnant patients to get vaccinated and boosted. If not for them, for their baby.
While 71% of pregnant people were fully vaccinated as of mid-July, a figure not much lower than national vaccination rates for people 18 or older, only around 2% received at least one of their shots while they were pregnant — suggesting that persuading people who are already pregnant to get vaccinated remains a challenge. Research points to a substantial waning in immunity five to eight months after getting the first vaccine, yet only 58% of pregnant people were boosted. Like with booster rates among those who aren’t pregnant, Black and Hispanic people trail behind.
Heerema-McKenney said obesity, high blood pressure, age and diabetes may also increase the risk of stillbirth, but, she said, it appears the strongest risk factor is not being vaccinated.
“We have a set of data saying that the vaccination is safe, and we have a set of data saying that COVID causes an increase in stillbirth. When you’re seeing those two,” she said, “to me it says, ‘Get the vaccine.’”
Another reason for optimism is that the height of SARS-CoV-2 placentitis appears to have coincided with the dominance of the delta variant; Heerema-McKenney said she has not seen a case of COVID-19 directly infiltrating the placenta for months.
Neither has Odronic, who is relieved to get back to her routine work of cancer biopsies after the punishing period last fall when she saw one to two stillbirths a week. Her hospital honored her in November as Physician of the Year for the “tireless leadership she demonstrated during the COVID response,” the first time the award was given to a pathologist.
But, doctors warn, the virus continues to mutate and the risk of stillbirth remains.
“Maybe we’re out of the woods with this, but we just don’t know,” Heerema-McKenney said. “There’s nothing more tragic than seeing a healthy pregnancy end because of something that’s potentially preventable.”
Back in southwest Ohio, doctors released Ginger from the hospital at the end of October, two and a half months after she was admitted. Her oldest daughter, Hailee, who is now 19, got vaccinated shortly after her mother was hospitalized. Ginger said she wanted to get vaccinated when she awoke in the hospital, but she said her doctors told her to wait a bit.
Since then, she said, her fear of the vaccine came flooding back.
At a recent appointment, Ginger listened carefully as her doctor urged her to get vaccinated, which, the doctor said, would be even more important if she were to get pregnant again. Ginger trusted her. “There’s no agenda behind it,” Ginger said. “I will get the vaccine.”
Ginger continues to wrestle with feelings of gratitude and guilt for surviving when her baby did not. In December, the family held a memorial service for the daughter they named Elliotte Jo and called Ellie. Ginger and Kendal were still too grief-stricken to speak, so Hailee and her uncle prepared remarks.
“You have the best dad that I know would have given you everything under the sun and protected you with every ounce of his being,” Hailee said. “And you also have the best mom to guide you through life. Having two older sisters, you would have had the best wardrobe and many visits to Starbucks.”
She breathed laughter into the room, if only briefly.
In June, the family traveled to Florida. As the waves lapped against the shore and the sunrise turned the sky pink, they etched Elliotte’s name in the sand.
The last thing people want to hear right now is that the coronavirus might have mutated yet again into yet another deadly variant, extending the pain, death, and inconvenience of a pandemic that we long hoped would be over.
However, whether the subvariant of omicron known as BA.2 will hit the United States as hard as it’s hitting other parts of the world is hard to say at this point, an expert at modeling the disease said Wednesday.
The pandemic has been full of unpleasant surprises and BA.2 is no exception. Scientists estimate that it’s one-and-a-half times as transmissible as the original omicron strain, BA.1, and is overtaking it.
Europe, and particularly the United Kingdom, have seen an increase in the new variant in recent months, but that hasn’t been the case everywhere, said Stephen Kissler, a research fellow in the Department of Immunology and Infectious Diseases of Harvard University’s T.H. Chan School of Public Health.
“The question of if and when a surge is coming and how large is very open,” Kissler said in a Zoom conference with reporters. “I know that we’ve seen surges that are dominated by BA.2 across much of Europe. But in contrast, for example, in South Africa we saw a major BA.1 wave — that’s where we saw the omicron wave first — and now there’s a lot of circulation of BA.2, but it hasn’t really caused an increase in cases so much that it’s lengthened the decline and given the epidemic a very long tail.”
Kissler explained that vaccination rates in the U.S. are lower than those in Europe, but higher than those in South Africa. That could mean that more Americans have developed antibodies against the omicron variants than have Europeans.
“To the extent that that gives us protection against BA.2 we might see dynamics that are more similar to what happened in South Africa,” he said.
Seasonality and other factors likely will play a role, Kissler said, with spring in the United States being a season of relatively low spread and fall a season of relatively high spread.
So if there is a surge here of the new variant, how will it affect Americans of varying ages?
“In many ways it will likely resemble our experience with COVID-19 up to this point,” Kissler said.
And past experience has shown one factor to be hugely important: vaccination.
Kissler said that being vaccinated, along with a booster dose, “really goes a long way toward helping to protect you from symptomatic disease and especially severe disease. The biggest delineation I imagine seeing is that people who are boosted will probably fare better than people who are unboosted.”
Another important factor is age, with the elderly having less natural resistance to all variants of the coronavirus than the young. Vaccines and boosters, though, can be a great equalizer.
“A vaccinated and boosted person over the age of 75, their risk is probably on the order of — if not lower than — an unvaccinated 20-year-old,” Kissler said.
COVID eventually will go from being a pandemic disease that spikes rapidly and overwhelms resources to an endemic one where a background level is present, sickening and even killing people, but in semi-predictable ways. Sadly, however, hopes that it will disappear altogether are small.
Looking forward, one simple public-health measure might be most effective, Kissler said.
“In many ways, one of the best things we can do to manage outbreaks is to just to continue to keep informing people how much COVID is circulating in their communities and make it just as accessible as a weather report,” he said. “A lot of data suggest that people tend to adjust their behavior accordingly.”
He said that probably won’t be enough to quell future waves of COVID, or be adequate in the face of major new variants.
“But as we continue to deal with COVID and we think about this permanent circulation of COVID-19 in the population — recognizing that there’s going to be different dynamics in different places, different patterns across the year — making it clear what’s happening in any given community at any given time through passive surveillance is probably the best thing we can do right now,” he said.
The coronavirus continued a five-week surge in Ohio on Thursday, with state data showing worsening infection and hospitalization rates.
While time lag and a Thanksgiving holiday cloud the latest data, an average of about 5,000 Ohioans per day contracted COVID-19 at the end of November, compared to about 3,600 daily at the beginning of the month, according to an analysis of state health department data.
Of any 100 tests taken over the last week, more than 15 on average are coming back positive — a nearly peak level of test positivity.
Hospitalization data reflects the case increase. About 190 Ohioans were hospitalized per day in late November, compared to about 145 at the beginning of the month. More than 3,900 state residents are currently hospitalized with COVID-19, according to data from the Ohio Hospital Association, the highest rate since early January.
Hospitalization rates are up for every age cohort besides those 0-19 years old.
Speaking to reporters Thursday, Ohio Department of Health Director Dr. Bruce Vanderhoff emphasized the best way to ease the hospital burden is to seek vaccination — vaccinated people comprise less than 6% of those hospitalized with COVID-19. Short staffed and fatigued hospital systems, he said, need the support.
“The problem right now isn’t necessarily physical beds and physical capacity, but staff,” he said.
In terms of vaccination, Ohio continues to fare poorly. The state is the 10thleast vaccinated in the nation, according to data from the New York Times. About 58% of Ohioans are at least partially vaccinated against COVID-19, compared to 71% of Americans.
Death data tends to lag behind infection data by several weeks, and there’s no clear picture of how many deaths resulted from the ongoing case surge. However, a previous case surge peaked in mid-September. By October, roughly 80 Ohioans per day on average died of COVID-19, despite widespread availability of safe and effective vaccines. Less than 5% of those who died of COVID-19 were vaccinated, per state data.
Ohio has yet to detect any cases of the Omicron variant, though it could be silently spreading. State health officials in Minnesota said Thursday they detected the new variant in a local man who recently traveled to New York City. The CDC announced Wednesday that health officials in San Francisco detected the variant in a person who had recently traveled to South Africa, where the mutation is believed to have originated.
With nearly 5,000 new cases of COVID per day, Ohio and the rest of the world are still dealing with a pandemic that started nearly two years ago. What we’ve barely begun to deal with, two experts said last week, is the long hangover many experience as “long COVID.”
That expression refers to a set of symptoms that linger for months after a person is infected with coronavirus. They include maladies of the lungs, heart, eyes, liver, brain, bladder, kidneys and pancreas. They also include problems of a less tangible nature, such as a loss of smell, chronic brain fog, headache and fatigue.
And, according to an October study published by the Journal of the American Medical Association, many, many people are likely affected by long COVID. The review of 57 studies found that more than half of the coronavirus patients followed were still suffering from symptoms of long COVID more than six months after they were infected.
With 78% having been hospitalized with COVID, that group appeared to have suffered worse infections than did the general population. Conversely, people who are fully vaccinated are far less likely to be hospitalized, and 49% less likely to develop long COVID, according to a study conducted in the United Kingdom.
Even so, the consequences of the condition are likely to be huge.
Ohio, for example, has seen more than 84,000 COVID hospitalizations, so it seems plausible that well over 40,000 Ohioans have suffered — or are still suffering — long COVID.
Nationally, “you’re talking about 30, 40, 70 million people,” Brett Giroir, who early in the pandemic was assistant secretary of the U.S. Department of Health and Human Services, said last week during a webinar organized by the National Institute for Healthcare Management Foundation.
As they were during the early days of the pandemic, policy makers are groping for ways to deal with long COVID without much in the way of scientific information to work with so far.
“We’re unfortunately dealing with from a position of a real lack of knowledge,” Walter Koroshetz, director of the National Institutes of Health’s Institute of Neurological Disorders and Stroke, said during the webinar.
“We’re really trying hard to understand what is the biological basis for the problems that people are experiencing and hoping to get some answers very quickly that can then be used to help patients,” Koroshetz added.
Giroir now is working with the health consulting firm Leavitt Partners on several issues, including problems related to the pandemic. He offered a broad framework for dealing with long covid.
“How do we organize the healthcare sector” in response to long COVID? he asked. “Do we have long COVID clinics. Do we have telehealth triage? How do we care for this 30 to 50% of 140 million people who potentially have long COVID?”
Giroir is proposing several steps to deal with the issue. Among them are helping medically underserved populations through grants to federally qualified health centers and primary-care practices, a national survey on the condition and by working to raise public awareness of it.
Governor DeWine announced today that the Ohio Department of Health has issued a “simplified” health order that “streamlines” previous orders into a single order that underscores the most important tenants of infection prevention.
“Our understanding of this virus and how it spreads is much more advanced than it was when we first learned about coronavirus in early 2020,” said Governor DeWine. “As we move to begin a new chapter in our fight against the pandemic, where more and more Ohioans are being vaccinated, this new order will focus on our best defense measures against COVID-19, such as wearing a mask, social distancing, limiting large gatherings, being outside, and practicing good hand hygiene.”
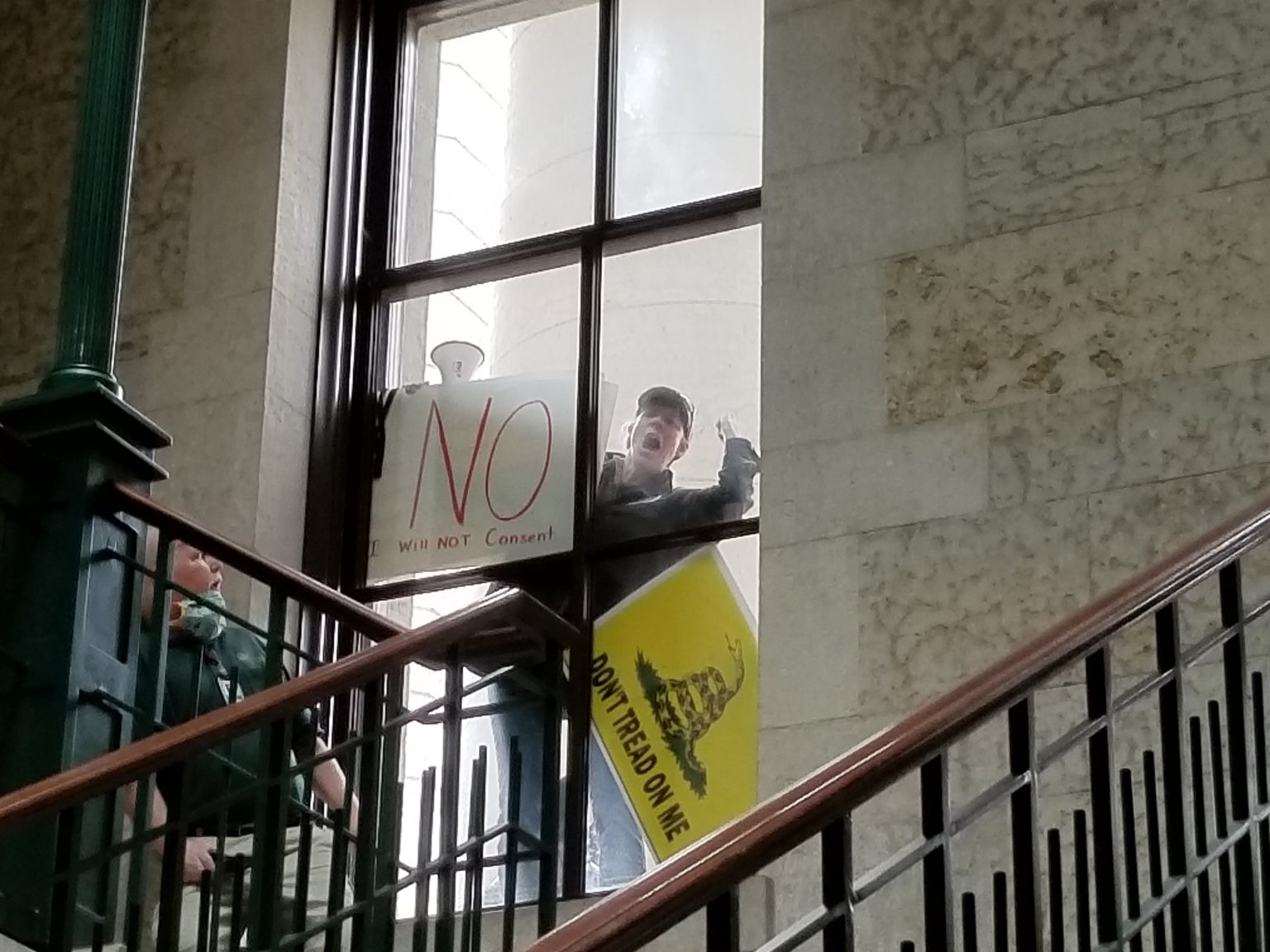
A man protesting Ohio’s health orders at the state Capitol on May 1. Gov. Mike DeWine later repealed most of them only to start reimposing orders on Tuesday as coronavirus cases continued to surge. Capital Journal photo by Marty Schladen
Ohioans were living with the coronavirus for about two months before GOP lawmakers initiated what would be a nearly yearlong effort to squash the state health department’s ability to issue public health orders.
The earliest version of the idea was to limit any order issued by the Ohio Department of Health to a two-week window. After that, a small panel of lawmakers would need to approve the order for it to stay in effect any further.
“We are clearly on the downside of the curve, there is no longer a risk of overwhelming the health care system,” said now-former Rep. John Becker to the House State and Local Government Committee, setting one of the first legislative attacks on the health department in motion via Senate Bill 1.
“I’m not sure there ever was, but that argument did make sense to me initially.”
A review of emails obtained by public records requests, committee hearings, interviews and contemporaneous media reports highlight just how absent public health was from efforts to wrest power from the health department during a pandemic.
In several instances, abortion politics, coronavirus infections among lawmakers, and overly rosy assessments of the pandemic from Republican leaders played a larger role in the legislation than the coronavirus itself.
SB 1 died an unusual death last May when every state Senator — even the bill’s sponsors — voted it down. Its supporters gave varying explanations from the Senate floor. They said it didn’t have an emergency clause, meaning it wouldn’t take effect for 90 days; and it was clumsily drafted.
Then-Senate President Senate President Larry Obhof, one of the most powerful Republicans in the state, later told constituents that Senators killed the bill, in part, because it could have expanded women’s access to abortion.
“A prominent Right to Life organization pointed out that the language, as written, could allow lawsuits challenging health orders that regulate or close abortion clinics,” he said in an email obtained in a public records request.
“Thus, the language could have been used to protect abortion clinics.”
The concern came from a letter the Greater Columbus Right to Life sent to lawmakers. Ohio Right to Life, which operates independently of the Columbus organization, disagreed, according to its director, Michael Gonidakis. However, he tried to stay out of it.
“We had no desire to be involved in that debate,” he said in a recent interview.
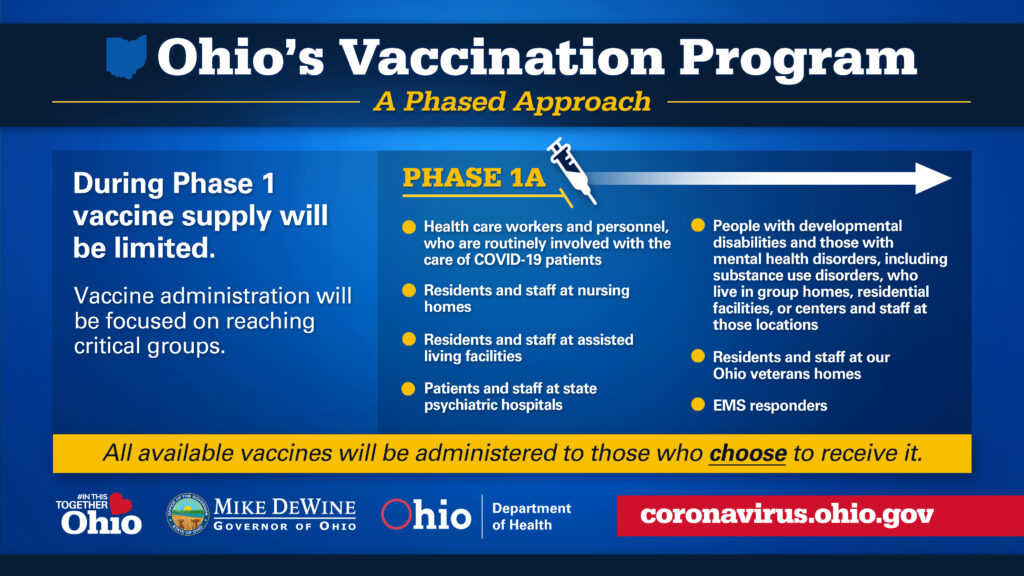
Loveland, Ohio – As more vaccine is produced more groups of people will be prioritized. However, it may be the middle of 2021 before the vaccine will be widely available to the Clermont County community.
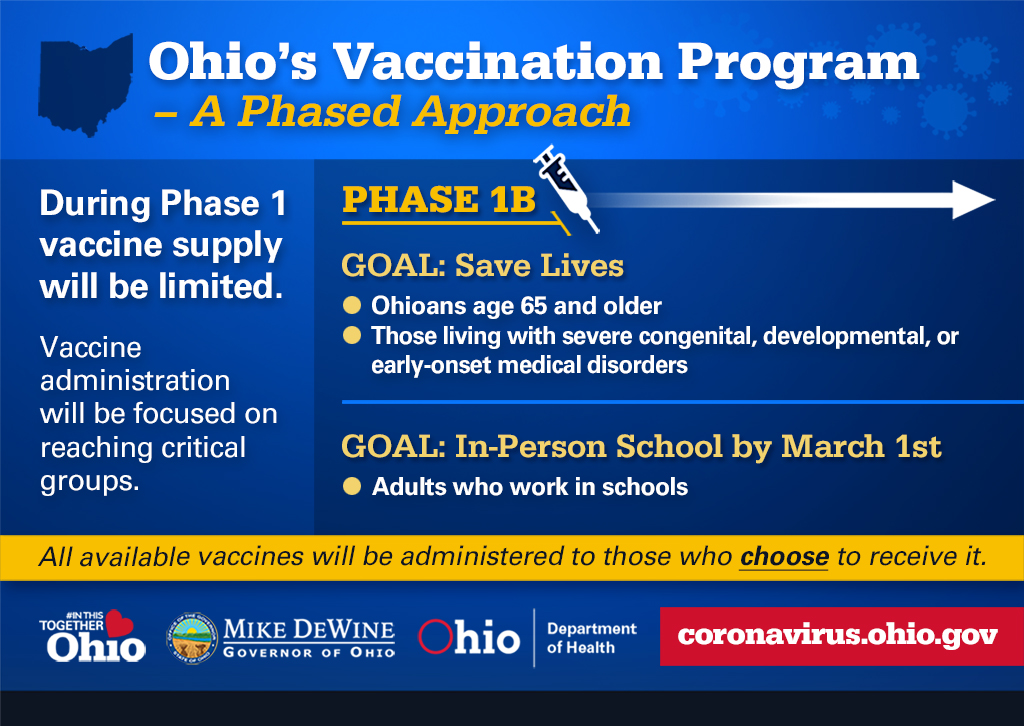
Beginning the week of January 18, Ohio will be vaccinating people who fall into phase 1B. That includes:
• Ohioans 65 and older • Those with severe congenital or developmental disorders • Employees of K-12 schools that wish to remain or return to in-person learning
Because the vaccine is still very limited in supply, Ohio will take a tiered approach to vaccinate group 1B. Ohio will follow this timeline for vaccinating group 1B.
Week of January 18 – Ohioans 80 years of age and older
Week of January 25 – Ohioans 75 years of age and older
Week of February 1 – Ohioans 70 years of age and older; K-12 school employees
Week of February 8 – Ohioans 65 years of age and older
If you or a loved one falls into group 1B and is eligible to be vaccinated, get on the:
Completing this survey will put you on the waiting list. A public health staff member will contact you to schedule an appointment or provide additional information about your vaccination options.
Heading into Election Day, Ohio appears to be in the midst of a sharp, broadly based spike in coronavirus cases with no end in sight, Gov. Mike DeWine said Tuesday.
Marty Schladen has been a reporter for decades, working in Indiana, Texas and other places before returning to his native Ohio to work at The Columbus Dispatch in 2017. He’s won state and national journalism awards for investigations into utility regulation, public corruption, the environment, prescription drug spending and other matters.
Continuing a trend, the 2,509 new cases reported from the previous 24 hours were a 27% increase over the 21-day average and the 198 new hospitalizations represented a 69% increase over the three-week average for that metric.
And as it is elsewhere in the United States, the virus is spreading into rural corners of Ohio that previously had been spared.
“Right now, 92.8% of Ohioans are living in a county that is high incidence and/or has very high exposure and spread,” DeWine’s office said in a tweet.
Adding to the alarm, the “positivity rate,” or the percentage of tests turning out to be positive for coronavirus, is nearing 6%. That’s about double what it was in late September.
Given the fact that Ohio continues to increase the number of tests that are administered, the higher rate indicates that people are spreading the disease to one another at a pace that is snowballing.
“We have no indication that we’ve plateaued out at all,” DeWine said during his Tuesday coronavirus press conference.
He said he found the situation so alarming that he was calling on medical, government, education and other leaders in each of the state’s 88 counties to work together on strategies to arrest the spread of the disease as cold, wet weather drives Ohioans indoors.
DeWine also had an appeal relating to Halloween and football parties and Thanksgiving gatherings.
“Please reconsider hosting gatherings of any size,” he said.
The dire statements brought the kinds of questions the governor has often faced since he started holding coronavirus briefings back in March.
One was whether he would reimpose orders closing businesses not deemed to be essential. Lt. Gov. Jon Husted said one reason such a move might be unnecessary is that much of the spread happening now in Ohio doesn’t seem to be occurring inside businesses.
DeWine also started to rule out the possibility of another shutdown but then seemed to think better of being too definite.
“We just can’t shut down twice, or we certainly don’t want to do it twice,” he said.
Then, after describing what could happen if the spread of the disease is unchecked, DeWine said things could get so bad that “we will one way or the other be shut down.”
DeWine also faced more questions about statements and actions concerning the pandemic by President Donald Trump and his staff.
One was a proposal to allow uncontrolled spread among populations without other health risks in an attempt to achieve “herd immunity.” If successful, it would mean that such a large chunk of the population would be immune to the virus that it would have a hard time spreading.
The idea has been endorsed by Scott Atlas, a doctor who doesn’t specialize in infectious diseases, but was placed on the White House coronavirus team after Trump saw him on Fox News.
DeWine echoed that on Tuesday, saying, “There’s no reputable scientist I’m aware of anywhere in the world” who thinks herd immunity can be achieved without a vaccine anytime soon.
DeWine was also asked why he greeted Trump at the airport Saturday. Trump was on his way to Circleville for a rally where people crowded together and at which Trump said the coronavirus is being overhyped by the media.
DeWine at first seemed to distance himself from Trump, saying he was merely respecting the dignity of Trump’s office. But then…
“Please understand exactly what it was. It was the governor of Ohio greeting the president of the United States,” DeWine said. “Again, I’ve also endorsed him and I continue to endorse him.”
Christopher Ball is a longtime Loveland resident and an attorney
by Chris Ball
Ruth Bader Ginsburg sat on the United States Supreme Court for 27 years. She authored countless judicial opinions on issues ranging from abortion rights, gender discrimination, and the landmark 2000 case of Bush v. Gore where she penned her now-famous line, “I dissent.” Justice Ginsburg passed away on September 18 from complications of pancreatic cancer. Her death lead to an outpouring of sadness, grief, and celebration of her icon status as a pioneer for the advancement of women’s rights and a brilliant jurist and lawyer.
As difficult as it is to do, the American political system must now decide how to proceed in the wake of the vacancy that now sits at the heart of the United States Supreme Court. Republicans and Democrats are forming the battle lines already, in advance of the election on November 3rd. The opening salvos have already gone out. The first one began even before Ruth Bader Ginsburg passed away.
According to Ginsburg’s granddaughter Clara Spera, the Justice dictated a statement to her that read: “My most fervent wish is that I will not be replaced until a new president is installed.” The fact that Ginsburg felt the need to utter these words when she knew she was in the last days of her life tell us all that we need to know about the importance with which she viewed the role of the Supreme Court in the coming years.
If the 2020 election is indeed a battle for the very future of this country, Ginsburg’s dying wish represents a call to arms in a battle to replace her in the country’s highest court, whose ability to shape law, policy, and affect the everyday lives of the American people has grown exponentially in the past half decade.
After initially stating that he would nominate Ginsburg’s replacement the week of September 21st, President Donald Trump pushed back the announcement out of respect for the former Supreme Court Justice’s family.
On Saturday Trump announced that he will nominate Amy Coney Barrett. Judge Barrett currently serves on the U.S. Court of Appeals for the Seventh Circuit, a position she was appointed to by none other than Trump himself.
Trump’s announcement that he would quickly push ahead and nominate a replacement sent Democrats into a frenzy of fervent anger and has kickstarted a non-stop news cycle that may even come dwarf coverage of the Coronavirus.
The questions are, how did we come to this, and what could happen if Trump’s nominee is appointed to the Supreme Court?
How we got here is harder to explain. Concerns about the power of the Supreme Court and the judges that comprise it have been hotly debated since it was created in 1789. However, the nomination process itself has often been something that gets overlooked when compared to the decisions that the Supreme Court hands down and the way it functions.
This all began to change in the late 1980s. In 1986 Antonin Scalia was confirmed in the Senate by a vote of 98-0. However, the failed nomination of Robert Bork in 1987 and the contentious confirmation of Clarence Thomas in 1991 changed the political landscape for Supreme Court nominees irrevocably. Of note, Joe Biden was the Chair of the Senate Judiciary Committee for both Bork’s and Thomas’ confirmation hearings and, as some argue, is the architect behind the transformation of the hearings into a “game of political revenge.”
Things only worsened in 2000. That election was so close that the Supreme Court was called upon to weigh in on Florida’s recount. In a razor-thin 5-4 decision the Supreme Court essentially held that George Bush was the victor in Florida, whose electoral votes were enough to win the day and the Electoral College, despite losing the popular vote by nearly half a million ballots. Polls at the time showed that the large swaths of the American people did not lose confidence in the Supreme Court after it decided Bush v. Gore. For their part, Democrats seemed more focused on the Electoral College and George Bush’s ability to win the Presidency despite losing the popular vote.
Another important development came about in 2013 and involved the “Nuclear Option” in the Senate. For decades, voting on Presidential judicial appointments (at any level) was by a super-majority in the Senate, or 60 votes. However, in 2013, Democrat Harry Reid invoked what was dubbed the “Nuclear Option” and lowered the threshold for approving Barack Obama’s appointments to a simple majority of 51 votes. Then, in 2017, Mitch McConnell had the votes to extend this “Nuclear Option” to the confirmation of Supreme Court Justices to confirm Neil Gorsuch’s appointment. Going forward, a nominee for the Supreme Court needed only 51 Senate votes for confirmation.
The Supreme Court and the confirmation process again came to national attention in 2016 when Mitch McConnell refused to even allow the Senate to consider Merrick Garland, Barack Obama’s nominee to replace the deceased Scalia. In a 2016 Opinion piece in the Washington Post, McConnell stated:
“Given that we are in the midst of the presidential election process, we believe that the American people should seize the opportunity to weigh in on whom they trust to nominate the next person for a lifetime appointment to the Supreme Court.”
He later went on to claim that the Senate had the power, under Article II, Section II of the Constitution to withhold its consent on the nomination. In his view, the Senate was right to do so since Barack Obama was in the final year of his second term, and 2017 would see a new President sworn in. Though Democrats were extremely unhappy with this act, there was little they could do to stop it.
Hillary Clinton’s 2016 loss to Donald Trump only cemented the belief in some Democrats’ minds that the very systems of elections and government in the United States were flawed on a fundamental level. The focus again centered on the Electoral College that allowed Trump to secure the Presidency despite losing the popular vote by 2.87 million votes. However, this time there was something else.
After Trump’s election, the American people seemed to pay more attention to politics and the national media scrutinized his every decision, tweet, and rally. This included his nomination of Brett Kavanaugh in 2018. More than 20 million people watched Kavanaugh’s confirmation hearing, which was “an audience size similar to that for a playoff football game or the Academy Awards.” His life and confirmation hearing were the focus of at least two books that were published in what seemed like real-time, as well as countless articles, opinion pieces, and more television panels than anyone can reckon. This was no doubt due to a confluence of the MeToo Movement, the allegations leveled against him, and the fact that Donald Trump was about to nominate his second Supreme Court Justice (after Neil Gorsuch in 2017). But with Kavanaugh, perhaps more than any other nominee in recent memory, there was a real argument about the fundamental function of the Supreme Court and the process that the President and Senate go through to appoint its Justices. Kavanaugh’s confirmation incited more than just ire from the Democrats, it only further confirmed their belief that now the Supreme Court, too, had become irrevocably corrupted.
Now, with the passing of Ruth Bader Ginsburg and the vacancy it leaves in the Supreme Court, in an election year, the political firestorm of judicial appointments and confirmation will again be at the center of our discourse.
But this time it will be different.
This is due largely to the confluence of several key factors, which include the Democrats’ disillusionment with the Supreme Court, the Electoral College, the recent contentious nomination proceedings in the Senate, and McConnell’s alleged hypocrisy in blocking a vote on Merrick Garland’s appointment while allowing one on Trump’s pick to proceed.
So what can the Democrats do if Trump’s nominee is confirmed?
While the Electoral College is frequent fodder for angry Op-Eds and it makes a nice sound bite for talking heads on television, the truth is that it is not going anywhere anytime soon. According to the American Bar Association and The National Archives, “over the past 200 years more than 700 proposals have been introduced in Congress to reform or eliminate the Electoral College” but none have been successful, for one simple reason. To eliminate the Electoral College would require amending the United States Constitution. Since this is unlikely to happen, there is one Constitutionally-recognized way that the Democrats could punish McConnell, Trump, and the Republicans.
Court packing.
Though the name sounds ominous and illegal, if the Democrats manage to win back the Senate, keep control in the House, and vote Joe Biden into office, it is a term that Americans should begin to get very familiar with.
The amount of justices on the United States Supreme Court isn’t fixed by the Constitution. All that Article III, Section I states is that “The judicial Power of the United States, shall be vested in one supreme Court, and in such inferior Courts as the Congress may from time to time ordain and establish.” This provision makes it clear that Congress is the branch of government that is to fix the number of justices on the Supreme Court.
The Supreme Court began with just six justices. Through various acts of Congress, the number has grown to as many as ten before settling to the current total of nine. History is replete with examples of how legislative acts have influenced the makeup of the nation’s highest court.
And that’s just what Democrats have threatened to do if Biden is victorious and they gain control of all branches of government in November. If Democrats control both houses and the Presidency, it is within their power under the Constitution to expand the number of Justices on the Supreme Court, just as Mitch McConnell has consistently stated that his efforts to block a vote on Merrick Garland and to obtain a vote on Trump’s replacement for Ginsburg are Constitutionally supported.
This is why McConnell, Trump, and other Republicans must be very wary of the way in which the voting public (especially independent and undecided voters) view their tactical decisions on this appointment. Current polls show that a plurality of Republicans actually favor waiting until after the election to replace the vacant Supreme Court seat. Susan Collins, a Republican facing a very tough re-election bid in Maine, issued a statement urging the same. Some Never-Trump Republican writers have advised cutting a deal with Democrats wherein Republicans would agree to hold off on naming a replacement in exchange for a promise that Democrats won’t add additional justices should they take the reigns of government in 2021.
However, with the recent announcement that Republican Senator Mitt Romney would, indeed, support a vote on Trump’s nominee, McConnell has likely secured all of the Senate votes he needs to push the process forward, and dashed the hopes of any kind of compromise on the issue.
As if the November election wasn’t already polarizing enough, the appointment and confirmation of Amy Coney Barrett could play a significant role in mobilizing voter turnout for Democrats. Their donors gave 42 million dollars in a single day following Ginsburg’s passing.
All signs point to Trump and McConnell successfully nominating a replacement for Ruth Bader Ginsburg, but they should be prepared for the potential fallout from Democrat and independent voters as well as for an expanded United States Supreme Court if they do.