The Ohio Department of Insurance provides Medicare beneficiaries with free, objective, health insurance information and one-on-one counseling through the Ohio Senior Health Insurance Information Program (OSHIIP). OSHIIP’s hotline experts, speaker’s bureau, and trained volunteers educate consumers about Medicare, Medicare prescription drug coverage (Part D), Medicare Advantage options, Medicare supplement insurance, long-term care insurance, and other health insurance matters.
_____________
Medicare 101 FREE at the Miami Township Public Library
Join us for our in-person “Welcome to Medicare” eventat the Miami Township Public Library.
If you will be eligible for Medicare soon and have questions, are helping a friend or family member navigate their Medicare benefits, or are currently on Medicare yourself and have questions or concerns, join us for this informative, helpful, in-person event!
Monday, February 10, 2025
6 PM
Clermont County Public Library – Miami Township Branch
Can’t make it to an event? Join us for one of the VIRTUAL (online) Medicare webinars or sign up for a one-on-one counseling session with one of our Medicare experts.
Can’t make it to an event? Join us for one of our VIRTUAL (online) Medicare webinars or sign up for a one-on-one counseling session with one of our Medicare experts!
You probably know someone covered by Medicare. Many people call OSHIIP to get information for their parents, grandparents, or other family members and friends who are covered by Medicare. If someone close to you is on Medicare, one way you can help is by taking the time to understand Medicare yourself. People covered by Medicare can get help from OSHIIP in various ways by:
Calling the OSHIIP hotline at 800-686-1578.
Talking with volunteers and contacting information sites near you.
Requesting a (virtual or in-person) speaker from our speakers’ bureau.
Reading our free literature.
[pdf-embedder url=”https://lovelandmagazine.com/wp-content/uploads/2025/02/Ohio-Senior-Health-Insurance-Information-Program.pdf” title=”Ohio Senior Health Insurance Information Program”]_____________
Contact the Ohio Senior Health Insurance Information Program (OSHIIP)
50 W Town St
Third Floor – Suite 300
Columbus OH 43215
WASHINGTON — Medicare can now negotiate lower prices for 10 common high-price drugs, cutting out-of-pocket costs for an estimated 9 million seniors and saving taxpayers billions, the Biden administration said Tuesday.
Medicare will begin this year to negotiate with the manufacturers of popular medications used to treat blood clots, diabetes, heart disease, rheumatoid arthritis, chronic kidney disease, psoriasis, blood cancers, Crohn’s disease, and ulcerative colitis.
Enrollees will begin to see lower prices in 2026.
The prescription drug negotiations are a result of last year’s Inflation Reduction Act, a massive spending package that contained measures to reduce prescription drug prices, subsidize climate change reduction technology and adjust the corporate tax rate.
“For far too long, Americans have paid more for prescription drugs than any major economy. And while the pharmaceutical industry makes record profits, millions of Americans are forced to choose between paying for medications they need to live or paying for food, rent, and other basic necessities. Those days are ending,” President Joe Biden said in a statement Tuesday.
About 9 million enrollees in Medicare’s Part D prescription drug coverage program spent $3.4 billion out of pocket in 2022 on the 10 drugs selected for negotiation, according to a report released Tuesday by the U.S. Department of Health and Human Services.
The 10 drugs are: Eliquis, Enbrel, Entresto, Farxiga, Imbruvica, Januvia, Jardiance, multiple Fiasp and NovoLog insulin products, Stelara and Xarelto.
Democrats hailed the announcement of the selected drugs. The party held majorities in both the House and Senate when Congress passed the Inflation Reduction Act along party lines in August 2022.
“For years politicians promised to take on the big drug companies and empower Medicare to negotiate lower drug prices for consumers. With the Inflation Reduction Act Democrats have delivered. Soon millions of Americans will see lower prices on some of the most expensive and widely used prescription drugs,” Senate Majority Leader Chuck Schumer of New York said in a statement Tuesday.
Sen. Jon Tester, a Montana Democrat, said in a statement that his constituents “should never have to make the choice between life-saving medication or putting food on the table.”
“I am proud to have stood tough against large pharmaceutical corporations and successfully demand that they stop unnecessarily jacking up prices on folks across the state. Montanans sent me to Washington to deliver results, and I will continue to take on anyone to lower costs,” he said.
Of the nearly 66 million Americans enrolled in Medicare, 52 million are enrolled in the Part D prescription drug coverage plan, according to the Centers for Medicare and Medicaid Services enrollment dashboard.
The Inflation Reduction Act also made common adult vaccines, including shingles and TDAP, free for certain Medicare enrollees. Monthly insulin costs for Medicare enrollees were also reduced to $35 for Part D beneficiaries as part of the IRA, and beginning in 2025 annual out-of-pocket prescription drug costs will be capped at $2,000.
The law’s prescription drug provisions, including the government’s new ability to negotiate what it pays for certain drugs, is expected to reduce the federal deficit by $129 billion by 2031, according to a Congressional Budget Office analysis.
The government will choose 15 additional Part D-covered drugs in 2025 to negotiate lower prices beginning in 2027. Several more Part D and Part B drugs will be phased in for negotiations through 2029.
ASHLEY MURRAY
Ashley Murray covers the nation’s capital as a senior reporter for States Newsroom. Her coverage areas include domestic policy and appropriations.
News from the U.S. Department of Health and Human Services:
The Centers for Medicare & Medicaid Services (CMS) is reminding people with Medicare that Medicare Open Enrollment began October 15, 2021, and now is the time to review their coverage options and make a choice that meets their health care needs. Medicare’s Open Enrollment period gives those who rely on Medicare the opportunity to make changes to their health plans or prescription drug plans, pick a Medicare Advantage Plan, or return to Original Medicare.
The Medicare Open Enrollment period occurs every year from October 15 through December 7, with coverage changes taking effect January 1. During this time, people can find a plan that better meets their needs, saves money, or both.
“This is an important time of year for 63 million Medicare beneficiaries across the country to compare coverage options to ensure they are getting the best benefits available at low cost,” said Health and Human Services Secretary Xavier Becerra. “We will continue to strengthen and build upon this critical program that has vastly improved the lives of our seniors. I encourage everyone to take stock of their health and find the best plan for them in 2022.”
Medicare plans can change year to year – even an enrollee’s current calendar year 2021 plan may have changes for 2022. Medicare.gov makes it easier than ever to compare coverage options and shop for plans. People can do a side-by-side comparison of plan coverage, costs, and quality ratings to help them more easily see the differences between plans.
“Medicare Open Enrollment is an important time of year for people with Medicare and their families to review their options and make choices about the health care coverage that best meets their needs,” said CMS Administrator Chiquita Brooks-LaSure. “It is also a time for people with Medicare to check their eligibility for Medicare Savings Programs, which can help with premiums and other costs. Enrollment assistance is available in your community and 24/7 at 1-800-MEDICARE to connect you to coverage that best fits your needs and budget.”
Here are some things to consider when shopping for Medicare coverage:
Check if doctors are still in-network and prescriptions are on the plan’s formulary.
Realize that the plan with the lowest monthly premium may not always be the best fit for specific health needs.
Look at the plan’s deductible and other out-of-pocket costs that factor into total costs.
Know that some plans offer extra benefits, like vision, hearing, or dental coverage, which could help meet individual health care needs.
Consider whether Original Medicare or a Medicare Advantage Plan is the best choice.
Medicare is Here to Help
Here are four ways you can compare plans and look at savings options:
Find plans at Medicare.gov and do side-by-side comparisons of costs and coverage.
Call 1-800-MEDICARE. Help is available 24 hours a day, including weekends.
Access personalized health insurance counseling at no cost, available from State Health Insurance Assistance Program (SHIP). Visit shiptacenter.org or call 1-800-MEDICARE for each SHIP’s phone number. Many SHIPs also offer virtual counseling.
Check eligibility for Medicare Savings Programs. People with Medicare facing challenges paying for health care may qualify for Medicare Saving Programs run by their state. These programs can help save money on premiums, prescription drugs, and other health care costs. If your income for 2021 is below $18,000, it may be worth contacting your state’s Medicaid program about help that may be available to you. Contact 1-800-MEDICARE to find out where to apply.
For more information, visit Medicare.gov or call 1-800-MEDICARE (1-800-633-4227). TTY users can call 1-877-486-2048. Help is available 24 hours a day, including weekends.
In response to the Food and Drug Administration’s (FDA) recent action that authorizes an additional dose of COVID-19 vaccine for immunocompromised individuals, CMS is assuring people with Medicare who qualify for an additional dose that they can receive it with no cost sharing. This is part of President Biden’s commitment that patients have access to the necessary vaccinations to protect themselves from COVID-19.
Medicare would pay for administering an additional dose of COVID-19 vaccines consistent with the modified FDA emergency use authorization (EUA) that was announced today. For COVID-19 vaccines administered on or after March 15, 2021, the national average payment rate for physicians, hospitals, pharmacies and many other immunizers is $40 to administer each dose of a COVID-19 vaccine. The Medicare program would continue to pay providers $40 to administer this additional dose – the same amount as paid for other doses of the COVID-19 vaccine.
CMS will share more information and guidance in the coming days about billing and coding for the additional dose of the COVID-19 vaccine for immunocompromised patients.
The Ohio Department of Insurance provides Medicare beneficiaries with free, objective health insurance information and one-on-one counseling through a program called the Ohio Senior Health Insurance Information Program (OSHIIP). OSHIIP’s hotline experts, speaker’s bureau, and trained volunteers educate consumers about Medicare, Medicare prescription drug coverage (Part D), Medicare Advantage options, Medicare supplement insurance, long-term care insurance, and other health insurance matters.
This article provided to Loveland Magazine was edited by David Miller and is by by Eye on Ohio, the nonprofit, nonpartisan Ohio Center for Journalism. Please join their free mailing list as this helps us provide more public service reporting.
In early March, just as Ohioans were learning about the first cases of novel coronavirus in the state, Anna Bondar’s grandfather fell at his Cleveland home.
Luckily, the 92-year old, who lives with dementia, wasn’t injured badly.
The tight-knit family started to discuss the possibility of a nursing home, though they had serious reservations.
Their tough choice was made even more difficult by mounting fears about the coronavirus. In nearly four months, COVID-19 has infected more than 31,191 people statewide and has proven particularly deadly for residents of long-term care facilities in Ohio.
Seventy percent of the reported deaths in Ohio due to COVID-19 complications have been in long-term care facilities, which is among the highest in the country.
Nationally the portion of COVID-19-related deaths in long-term care facilities has hovered just over 40%, though the amount of testing done in nursing homes varies significantly by state.
Every day, families like Bondar’s are making what can feel like an impossible choice – whether to send a loved one to a nursing home where they will receive around-the-clock specialized care but face a greater risk of contracting COVID-19, or to care for that person at home where risk of transmission is lower but providing care can be more challenging.
Even before the pandemic, sorting through the myriad of quality ratings and measures was daunting enough. Then, COVID-19 deaths started to soar.
Now, families and seniors agonize over what could be life or death choice using confusing numbers on infection “hotspots” and without the ability to visit nursing homes to observe how the staff cares for residents – which is the number one recommendation of most advocates.
Dr. Amy Acton, director of the Department of Health
State officials, including Dr. Amy Acton, the former director of the Department of Health, have emphasized that “congregate” settings like nursing homes are at highest risk of infection. Staff, who often travel between facilities, need to be in close contact with residents to provide care. And residents, who are primarily older and have multiple medical conditions, are more susceptible to COVID-19-related complications.
“All of this makes it high risk. At the same time, it’s really necessary for many patients to be there,” said Dr. Steven Schwartz, a geriatric physician at the Cleveland Clinic who travels to nursing homes as part of the Clinic’s Center for Connected Care.
Ohio National Guardmembers will begin testing all staff members and any residents who likely were exposed to COVID-19 in the state’s nursing homes, Gov. Mike DeWine announced May 27. What are being called Congregate Care Unified Response Teams will focus on facilities where confirmed or assumed positive cases are reported in hopes of reducing the number of COVID-19 cases and deaths in Ohio’s nursing homes, which as of May 27 was 5,324 resident cases and more than 1,442 deaths.
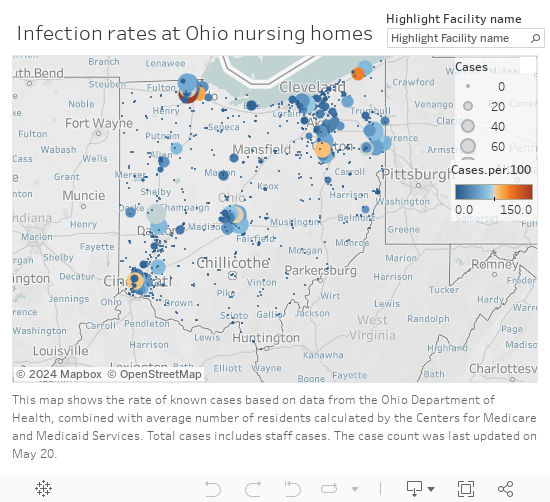
Infection rates in Ohio Nursing Homes
Making an educated decision
Last month, state officials began to release the numbers of reported infections and deaths in long-term care facilities, which include nursing homes, rehabilitation centers, and assisted living centers.
But it’s unclear how much the numbers – which are reported weekly and are also tracked cumulatively – matter for families currently trying to choose a facility.
The state, on its coronavirus website, says the infection and death numbers shouldn’t replace a thoughtful conversation with a nursing facility about infection control practices and that “residents and family members should understand that the presence of COVID-19 at a facility is [in] no way an indicator of a facility that isn’t following proper procedures.”
Yet many in the health care industry say infection information should be considered, along with other factors, when deciding which site to choose.
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck.”
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck,” said Dr. James Campbell, department chair of geriatric medicine at MetroHealth.
The infection information provided by the state can be useful, for instance, if a family is choosing between two similar facilities, said Nate Cyrill, a Long Term Care Ombudsman for Cuyahoga, Geauga, Lake, Lorain and Medina counties.
Since information on the virus changes rapidly, most families still rely on the quality measures that were available before COVID-19, including existing state and federal online guides Cyril said.
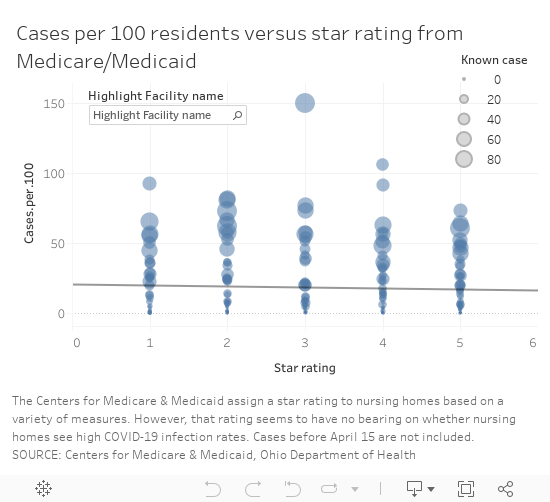
One of the commonly-used ranking systems, maintained by the Centers for Medicare and Medicaid Services, assigns ratings – from 1 to 5 “stars” – to facilities based on performance on quality measures, staffing and inspections.
The number of “stars” Ohio’s nursing homes received, however, does not appear to have a correlation to the number of infections reported to the state, based on a comparison of the publicly available information. The analysis did not include assisted living facilities.
Cases vs. Star rating
“You want to look for a nursing home that’s four of five stars preferably but even that doesn’t tell you the whole story,” Steven Schwartz said.
There are numerous 1-star rated facilities that have reported few infections, like Whetstone Gardens and Care Center in Columbus, which has reported 9 cases or 8 per 100 residents.
Salem North Healthcare Center
Salem North Healthcare Center in northern Columbiana County had 51 patients test positive for the virus as of May 20, as well as five staff, according to the state. It is rated a 5-star facility, the highest rating from CMS.
It’s one of four 5-star facilities with an infection rate over 50 casesper 100 residents, based on Medicare’s calculation of each facility’s average number of residents. (The rate does not include infections among staff because the number of staff in each facility was not available.)
Since April, the focus on high numbers of reported infections, often referred to as clusters, in long-term care facilities has intensified. In some cases, those numbers are a reflection of the level of testing, said Fred Stratmann, general counsel and chief compliance officer for CommuniCare Health Services. It doesn’t mean all of the residents with a positive test had symptoms of COVID-19. The state infection numbers also don’t show the residents who have recovered from the virus, he said.
CommuniCare, which operates close to 90 health care facilities in seven states has been proactive about testing, Stratmann said. When COVID-19 cases started to appear at the North Salem facility, the company enlisted the state’s “strike team” to proactively test all of the residents. It has since re-tested all of the residents who were initially negative and purchased 3,000 testing kits to supplement what the state could provide.
“We wanted to be certain of the extent of COVID in this center in order to be able to properly treat it and to fight back against it,” Stratmann said. The facility does that by isolating any COVID-19-postive patients in a separate unit with its own dedicated staff and by admitting new residents to an observation unit for 14 days to make sure they have no symptoms of infection, he said.
Restrictions on visits make choices harder
The most effective way to scout out a facility typically is to visit it, preferably unannounced, said Dr. James Campbell, department chair of geriatric medicine at MetroHealth. However, because visitors aren’t permitted in nursing homes right now, the next best thing is to ask detailed questions about care, any COVID-19 cases and infection control measures, he said.
Campbell also suggested turning to hospital staff, who work with nursing homes regularly, for advice. Social workers can place five people in a week, while most individuals face that decision, at most, only a few times in their lives, he said.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
The agency, along with other similar independent agencies across the state, investigates complaints in long-term care, skilled nursing, group homes and rehabilitation facilities and can share what are called “verified complaints” that aren’t otherwise available publicly.
Most of the complaints investigated in relation to COVID-19, Cyrill said, have been related to visitation or the ability of families to get information on a loved one’s condition.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
Under normal circumstances, an ombudsperson would go to the facility and talk to patients and could do so without announcing the visit in advance. Since visits are restricted for infection control reasons, they have to work through staff to speak to residents or to ask questions, which isn’t optimal. And they aren’t able to make direct observations.
“It makes our job much more challenging,” Cyrill said.
At the North Salem facility, which has had about a dozen new residents admitted or transfered from other facilities, the staff has given “virtual tours” over the phone to family members or prospective residents who were in the hospital, Stratmann said. The company also invested in technology that won’t replace face-to-face visits but enables more family contact and the ability and for staff to help keep residents’ spirits up by making videos of activities, like dancing and singing, to keep them connected with the local community.
In addition, Stratmann said they walk families through the infection control procedures and share techniques they have implemented to improve health outcomes for patients with COVID-19 including, when appropriate:
Treating residents with anticoagulant medications to reduce the risk of blood clots and strokes, which has been a factor in some COVID-19-related fatalities.
Practicing “proning” or positioning residents, while awake, flat on their belly and chest to reduce the buildup of fluid in lung tissue and reduce the risk of Acute Respiratory Distress Syndrome, which has been associated with many COVID-19 fatalities.
The idea of putting their beloved grandfather in a nursing home was gut-wrenching
Choosing home
For Bondar’s family, the idea of putting their beloved grandfather in a nursing home was gut-wrenching, especially as visitation was curtailed to limit the virus’ spread. He speaks Russian, his native language, and would not have been able to communicate well with the staff caring for him.
“It felt like admitting him [to a facility] would be like saying goodbye,” Bondar said. “Like leaving him to die.”
Bondar’s family ultimately decided to care for her grandfather at home, in his Mayfield Heights senior highrise, where they could limit his exposure to the virus.
Before his fall, an aide visited for about eight hours a week. After the Ohio’s “stay at home” order was put in place March 23, Bondar and her mother were able to work from home and pitch in with care.
The advice of the Clinic’s Steven Schwartz led them to a hospice program, which helped the family find additional aides, including one who speaks Russian, as well as a hospital bed for safer sleeping and a wheelchair.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
“We’ll do this as long as we can manage it,” Bondar said.
Anecdotally, it is a choice more families are making: the decision to use home care or even pull family members out of nursing homes out of fear or because they miss them and can’t visit, Steven Schwartz said.
“Sometimes it’s appropriate. But sometimes, even given everything, it may be safer to have your family member there to get stronger and get the necessary care,” said Steven Schwartz. “I would really try to balance the benefit of going to a nursing home versus the risk.”
Patients with dementia or Alzehimer’s may be unsafe going back home.
Patients with dementia or Alzehimer’s may be unsafe going back home, he said, and families may need to decide if a nursing home really is the safer place.
One of the first orders Ohio put in place to prevent the spread of COVID-19 was to halt in-person visitation in more than 900 nursing and long-term care facilities. The state is not yet ready to lift those restrictions and resume visits in those settings, Gov. Mike DeWine said, but on June 8 will start allowing outdoor visits at assisted living facilities care centers for individuals with disabilities.
“We are not to nursing homes yet and I know that causes anguish for a lot of people who are watching this but we’re trying to do this so that we don’t increase the COVID inside the nursing homes or the assisted living or the immediate care facilities,” DeWine said during a May 28 briefing.
Decisions made harder
Figuring out what kind of care might be best for a patient has become more challenging, too.
Previously, nurses and social workers would visit clients in their homes to assess how they functioned – whether they could independently bathe, cook and grocery shop, said Theresa Foster, a nurse and licensed social worker at Western Reserve Area Office on Aging.
They relied on conversations with clients and family and also observations of the environment in the home and possible risks, said Foster, who runs the agency’s resource center.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Now, those assessments are done by phone and can be done successfully, but it is more difficult, Foster said.
At UH’s hospitals, medical staff use a scoring system to determine the best place for a patient being discharged, said Dr. Sean Cannone, UH’s medical director for population health.
Patients are assessed on their ability to perform daily tasks and on their cognitive abilities.
“We’re trying as much as we can to get patients home if at all possible,” he said. The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
“We want to respond to what people really want for their own care,” Cannone said.
The shift started before COVID-19 cases surfaced but has accelerated as more families worry about potential exposure to the virus in congregate living situations.
As technology has advanced, the capabilities of what can be done in a patient’s home has also increased. In March, UH introduced a new patient management system, Massimo SafetyNet, for remote monitoring.
When patients are released from the emergency room or from a COVID-19 floor, providers now put a bluetooth sensor on their wrist — it looks like an Apple Watch — that streams data about a patient’s vitals to a central monitoring center, said Jonathan Sague, UH’s vice president of clinical operations. That way, providers can make sure a patient is safe at home.
Douglas Beach is the chief executive officer at Western Reserve Area Office on Aging
Douglas Beach, chief executive officer at Western Reserve Area Office on Aging, has had firsthand experience weighing care decisions amid COVID-19 worries. His mother is rehabilitating in a nursing home after a six-week hospital stay related to a heart condition.
Not being able to visit her in the hospital or the facility has been hard, Beach said. He and his brother, who is a doctor, had to make all of the arrangements by phone, including figuring the best way to transport her that would have the lowest risk of exposure to the virus.
“Home and community-based services is what I do,” Beach said. Part of his mission is to advocate for the setting that allows for any person, whether they are older adults or live with a disability, to be as independent as possible .
But for his mother, a nursing facility was the right choice because she needed 24-hour care that her family could not provide at home.
Beach said nursing homes have had to deal with an unprecedented set of circumstances: a new virus, initial unknowns about transmission and populations at extremely high risk for complications.
Nursing homes will continue to play a vital role and will remain the best option for people who need more care than can be safely provided at home, Beach said.
For the more than 9,500 clients his agency serves in Cuyahoga, Geauga, Lake, Lorain and Medina counties, delivering care at home, with health aides, nurses and community and family supports, has proven a low risk. As of mid-May only 35 clients had tested positive for the virus, he said. That is roughly 0.3% of clients, though not all clients are tested.
Managing COVID-19
Cuyahoga County nursing homes have been paired with one of the area’s three largest hospital systems during the pandemic, Campbell said. The hospitals help the facilities both prepare for and respond to COVID-19 cases.
“The goal is when you have one patient in a nursing home with COVID is to make sure you don’t end up with 30 patients with COVID,” Campbell said.
UH developed what is being called a playbook for local nursing homes. The playbook gives facilities a plan for how to respond if there’s a COVID-19 outbreak on-site, said Sague, who works as a firefighter and medic on the weekends.
“It can be pretty startling and pretty alarming if they’re not ready for it,” Sague said.
The playbook gives guidelines on screening, triaging, determining exposure, testing and isolating those who test positive, as well as how to get personal protective equipment, increase staffing and to eventually reopen safely, Sague said.
Once a case is identified at a facility, what is known as an intercept team is dispatched — either virtually or in person — to help a nursing home handle it, he said.
Patrick Schwartz, director of strategic communications for LeadingAge Ohio, a long-term care trade association, said access to testing and safety equipment has been a consistent problem for Ohio’s nursing homes.
But in the past month or so, the state has made “a definite shift” and started prioritizing testing at nursing homes, which is helping, he said.
Patrick Schwartz said he hoped the expanded testing would enable facilities to test their entire population— of residents and staff — so they can better limit the spread of the virus.
Throughout Ohio, populations that have received mass testing — health care workers, first responders, those incarcerated and those in nursing homes — have had higher numbers of positive cases. Many people with COVID-19 are asymptomatic, so it is unknown if they have the virus until they are tested.
“Since this pandemic first reared its head, it was clear to long-term care providers that the front lines would be in long-term care,” Patrick Schwartz said. The populations at those congregate living facilities, many of whom are older and have multiple medical conditions, are among the most vulnerable for complications from COVID-19, he said.
In Cuyahoga County, and elsewhere, local health departments have deployed limited testing resources to nursing homes quickly in hopes of limiting spread in and between facilities and given guidance to homes about how to isolate patients and trace exposures between facilities to limit the spread of infection.
Cuyahoga County Health Commissioner Terry Allan said nursing homes try to guard against outbreaks but have varying degrees of resources. The assistance from the National Guard will allow more residents and staff at facilities in Northeast Ohio to be tested, he said.
Support for this project was provided by the Center for Community Solutions.
Questions to ask:
How can family members stay in touch with residents while visiting is restricted?
Does staff facilitate video visits? Is window visiting allowed?
How often will the facility provide updates on a resident’s condition?
How much COVID-19 testing is being done? Is the facility proactively testing patients or only those with symptoms?
Are private rooms available?
Do staffing ratios allow for residents to be taken outside?
Are residents currently restricted to rooms?
Are separate units and staffs used for COVID-19-positive patients and COVID-19-negative patients?
How does the facility work to limit COVID-19 complications?








 Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services. 

