Below are some of the top findings from the release.
Suicide is a leading cause of death for working-age Ohioans.
Over 1,400 Ohioans died from suicide in 2022, the most recent year we have data for. This makes suicide the fifth-leading causes of death for working-age Ohioans, behind unintentional injuries like drug overdose and motor vehicle crashes, cancer, heart disease, and COVID-19.
Ohio’s suicide death rate is 15 deaths per 100,000 people, just slightly above than the national rate of 14.5 deaths per 100,000 people.
Suicide victims are disproportionately white, male, working-age, and Appalachian.
In 2022, 17 white Ohioans died from suicide per 100,000 population, higher than the rate of 12 for Black Ohioans, 10 for Hispanic Ohioans, and 7 for Asian Ohioans. Men were also four times likely to die from suicide than women. This is despite the fact that women attempt suicide at a rate 70% higher than men.
Suicide rates were highest in 2022 for working-age adults, higher than the rate for young adults, retirement-age adults, and children. Suicide was most common in Appalachian counties, with 15 of Ohio’s 22 counties with the highest suicide rates located in Appalachia.
Suicide is on the rise–for nearly everyone.
Since 2007, suicide rates have increased for men and women, white, Black, and Hispanic Ohioans, and Ohioans in every age group. The only major demographic group that has seen a flat suicide trend are non-Hispanic Asian or Pacific Islander Ohioans.
Risk factors for high school students are also becoming more common.
Compared to 2019, female Ohio high school students were more likely in 2021 to feel sad or hopeless, seriously consider suicide, make a plan to commit suicide, or attempt suicide. While more male high-school felt sad or hopeless and seriously considered suicide over that time period, fewer made a plan or attempted suicide. The increase in suicide plans and attempts among female students was much larger than the decrease among male students.
The increase in suicide rate is driven by firearms.
Suicide deaths involving a firearm increased 60% from 2007 to 2022. This accounted for 75% of the total increase in suicides over that time period. The remainder of the increase was driven mostly by an increase in deaths by suffocation and other causes. Deaths by poisoning decreased over that time period.
Suicide is a hard social problem to make progress against. That being said, the Health Policy Institute of Ohio suggests interventions to improve mental health to prevent suicide attempts.
A 2016 evidence review published in the American Journal of Psychiatry concluded legislation reducing firearm ownership lowers firearm suicide rates. It also acknowledged, however, that court interpretations of the second amendment to the U.S. Constitution have made most legislative options for reducing firearm ownership politically unfeasible in the United States.
The researchers however, say targeted initiatives like gun violence restraining orders, smart gun technology, and gun safety education may be able to reduce risk for current gun owners. These sorts of approaches do not have a strong evidence base yet, but they at least give us something to tackle this difficult problem.
If you or someone you know needs support now, call or text 988 or chat 988lifeline.org.
ROB MOORE
Rob Moore is the principal for Scioto Analysis, a public policy analysis firm based in Columbus. Moore has worked as an analyst in the public and nonprofit sectors and has analyzed diverse issue areas such as economic development, environment, education, and public health. He holds a Master of Public Policy from the University of California Berkeley’s Goldman School of Public Policy and a Bachelor of Arts in Philosophy from Denison University.
In an effort to increase the number of Ohioans who currently have not taken a COVID-19 vaccine to get vaccinated, Governor DeWine announced a series of statewide drawings to help incentivize vaccinations.
Ohioans under the age of 18 who are eligible to receive a COVID-19 vaccine will be entered into a drawing for a four-year full scholarship to any of Ohio’s state colleges and universities, including full tuition, room, and board.
Ohioans aged 18 and older will be entered into a weekly drawing with a prize of up to $1 million.
A total of five weekly drawings for each prize will take place, with the first winners being announced on May 26th. Winners must have received at least one dose of a COVID-19 vaccine by the date of the respective drawing.
The drawings will be administered by the Ohio Department of Health, with technical assistance from the Ohio Lottery Commission, and will be funded through existing allocations to the Ohio Department of Health of unexpended coronavirus relief funds.
Further details and contest rules will be announced by the Ohio Department of Health and the Ohio Lottery Commission next week during a briefing to news media.
One month ago, nearly 475,000 Ohioans over seven days marched into small pharmacies and mass clinics alike around the state to get vaccinated against COVID-19.
Each week since, the number of newly “vaccine-started” Ohioans has tumbled. Just 152,000 Ohioans were vaccinated during the week ending April 25, according to data from the Ohio Department of Health.
As the vaccine rollout pace slows, only about 4.7 million of Ohio’s 11.7 million residents have begun the vaccination process.
“We clearly have a lot more vaccine than we have demand,” Gov. Mike DeWine said to reporters Monday.
Vaccines protect individuals against COVID-19 but, at a certain threshold, can protect those in a population who haven’t yet or cannot receive the vaccine. Experts have estimated this threshold, known as herd immunity, to be somewhere between 70% and 90%.
While the first four months of the vaccine rollout were defined by scarcity, uptake rates began to plunge nationally in April.
DeWine, noting the uptake has declined “dramatically,” said herd immunity is more of a gradient than a black-and-white concept. The formula, he said, is simple.
“The more people that get vaccinated, the harder it is for this virus to spread,” he said. “The more people that get vaccinated, the fewer people that are going to die.”
All told, more than 19,200 Ohioans have died from COVID-19, and nearly 57,000 have been hospitalized. The Ohio Department of Health reports more than 1 million residents have been infected, though the true count is likely much higher.
Ohio is in the middle of the pack in terms of states and percentage of the population who have received at least one dose.
On the low end: Mississippi (31%), Louisiana (32%), Alabama (33%), Wyoming (34%) and Idaho (34%) according to New York Times Vaccine Tracker data.
On the upper end: New Hampshire (61%), Massachusetts (58%), Vermont (57%), Connecticut (56%) and Maine (55%).
The U.S. Census Bureau has been surveying Americans’ attitudes about the COVID-19 vaccine. As of March 29, nearly 20% of Ohioans expressed hesitancy toward the vaccine, compared to about 15.6% nationally. The bureau is slated to release fresh data later this week that will give a sense of whether the trend is improving or worsening.
Similarly, polling data from Kaiser Family Foundation estimates 13% of Americans will “definitely not” get the vaccine and another 7% only will if they’re required to. Other data from Gallup estimates that 26% of Americans are unwilling to take the vaccine, down from about 35% when they were authorized for use in December.
Ohioans struggling to pay their rents or mortgages may head into 2021 without the housing protections and public assistance that have carried them through much of the pandemic this year.
A federal moratorium on evictions is about to expire. Two other relief programs helping unemployed Americans are set to run out. There are believed to be thousands of Ohioans who are in immediate risk of eviction due to unpaid rent, with many low-income earners still working reduced hours or remaining out of work entirely.
Back in March, two Democratic lawmakers proposed a statewide moratorium on eviction and foreclosure actions so long as Ohio stayed under a state of emergency amid the COVID-19 pandemic. The economy has rebounded somewhat from historic unemployment in the spring, but the virus outlook looks grim as the state heads into the cold winter months.
State Reps. David Leland of Columbus and Jeffrey Crossman of Parma believe the moratorium is needed now more than ever.
“This is not just a humane thing to do,” Leland said in a committee hearing on the bill Thursday morning, “it’s not just asking you to embrace the holiday spirit. Instead, as we survey the landscape after these tumultuous nine months and ahead of next year’s budget negotiations, this is a way to save numerous low-income Ohioans’ from unimaginable hardship.”
“The urgency of this legislation is really right now,” Leland continued.
Under House Bill 562, landlords could still file eviction actions, but courts would be prevented from acting on them while the state of emergency is in place. Law enforcement officers could not carry out eviction orders either. Courts would not be able to conduct any business pertaining to foreclosures and must halt all pending foreclosure actions.
This moratorium would apply to residential and commercial properties.
Nearly two-dozen Democrats and one Republican have supported the bill as cosponsors.
iStock / Getty Images Plus
‘Last remnants of the safety net’
The large-scale CARES Act signed into law in March has provided trillions of dollars of relief, but many of its programs benefiting Ohio tenants have already run out or are about to.
This includes the Pandemic Emergency Unemployment Compensation and the Pandemic Unemployment Assistance programs, which have helped those who have lost work during the crisis. Both programs end the day after Christmas.
In September, the Centers for Disease Control and Prevention (CDC) issued a nationwide moratorium on evictions for residential properties. It prohibits U.S. landlords and property owners from evicting a tenant for unpaid rent.
That moratorium is set to expire on New Year’s Eve.
“Just as covid cases are exploding and our hospitals are filling, and just as the coldest parts of winter are setting in, hundreds of thousands of Ohioans are set to be stripped of the last remnants of the safety net Congress put in place back in March,” Leland said.
Ohioans struggled to pay their housing costs even with that safety net in place. A survey from this past summer found more than a half-million residents could not pay rent in June 2020.
Now these same residents potentially face 2021 without the CDC moratorium and without relief assistance — unless Congress acts again to pass a relief bill to close the gaps left by the still struggling economy.
A total of $50 million from the CARES Act was allocated for emergency rental assistance in October. But advocates say more is needed.
“Unless the Senate stops blocking any meaningful relief, we’re really worried about what’s going to happen in 2021,” said Marcus Roth, a spokesman for the Coalition on Housing and Homelessness in Ohio, last month.
That’s also the hope of Gov. Mike DeWine, who again called on Congress to pass a relief bill during his COVID-19 press conference on Thursday.
DeWine was asked if he supported the CDC extending its eviction moratorium into 2021.
“I’d have to take a look at that. I don’t know,” DeWine answered. “But look, this is a problem. This is a problem and is something that we are in fact focused on.”
Lt. Gov. Jon Husted argued that a moratorium alone does not address the costs faced by property owners and suggested such action should be paired with further government relief.
“There’s still somebody that has a mortgage to pay on that facility, who has a default that could potentially happen with their lender, which creates a whole chain of events and series of events,” Husted said. “So there has to be a financial solution to go along with any moratorium so that we don’t create a chain reaction in the system that causes additional problems.”
Unintended consequences to a moratorium?
In committee, state Rep. D.J. Swearingen, R-Huron asked the HB 562 sponsors about the “unintended consequences” of continuing a moratorium in Ohio. Swearingen noted that property owners still have costs such as repairs and that smaller banks may not be able to carry so many unpaid loans.
State Rep. D.J. Swearingen, R-Huron
Crossman acknowledged those concerns but said the ramifications of doing nothing would have a greater impact on individuals.
“I think we just have to ask ourselves, who’s in a better position to bear the burden here? The individual who is not making any income trying to keep their family fed and clothed and in a housing situation during the middle of a pandemic, particularly if they don’t have a job, or a lender who can maybe take a two- or three-month pause from getting their mortgage payments?”
Crossman said the latter is in “a far better position financially” to handle the issue.
Lawmakers also heard testimony from Dan Acton, a lobbyist for the Ohio Real Estate Investors Association who spoke in opposition to passing an Ohio moratorium. He said his organization consists of a few thousand “smaller” real estate investors who typically own single-family housing units.
He claimed these property investors operate on “razor-thin profit margins.” When tenants do not pay their rent bills, Acton said, this reduces the “profits for a property owner that could otherwise be used to reduce the overall debt on a property or make improvements.”
“The pandemic and the resulting eviction moratoria and payment delays are leaving our members on the brink of failure,” Acton said, arguing it would be “dangerous” for the government to “interfere” with a private leasing contract.
Leland said a moratorium is not meant to be a “long term-solution,” but would allow Ohioans to stay in their home until winter passes, the economy rebounds and a vaccine is made available.
Separately, Leland and fellow Democratic Rep. Juanita Brent of Cleveland also sponsored House Bill 744 that would allocate around $270 million from the state’s “rainy day fund” to pay for a new COVID-19 Emergency Rental Assistance Program. No action has been taken on this bill.
Marty Schladen has been a reporter for decades, working in Indiana, Texas and other places before returning to his native Ohio to work at The Columbus Dispatch in 2017. He’s won state and national journalism awards for investigations into utility regulation, public corruption, the environment, prescription drug spending and other matters.
Ohioans seem to be living in two realities. Coronavirus cases are soaring, but many refuse to acknowledge it.
Spoiler alert: President Trump might have something to do with the dissonance.
Ohio got some of its worse coronavirus news to date on Thursday, with Gov. Mike DeWine reporting yet another record in cases over the past 24 hours — 2,425— along with an alarming increase in hospitalizations due to the disease.
And as he reported those numbers in his covid press conference, DeWine invited some sobering testimony from a prominent covid sufferer.
“It’s like getting beaten up from the inside out,” former New Jersey Gov. Chris Christie said via Zoom, describing his recent bout with coronavirus that landed him in the intensive-care unit for six-and-a-half days.
Go to the 6:10 minute mark of the news conference to watch the Zoom call between former New Jersey Gov. Chris Christie and Gov. Mike DeWine. (Video: The Ohio Channel)
Christie described the isolation of lying alone in a room, communicating with hospital workers by white board through two-inch glass and not knowing whether he’d ever make it out.
“That combination of physical and psychological stress was pretty unique in my life and pretty extraordinary,” he said. “I can’t emphasize enough: I know how tired everybody is… But as tired as you are of strapping that mask on or going to the sink and washing those hands again, I can tell you, you will take those days in a heartbeat compared to getting this disease.”
Yet at the same time, people living in a very different reality were expressing themselves on DeWine’s Twitter feed.
Some were falsely arguing that the fall spike in cases is proof that wearing masks doesn’t mitigate the spread of the virus. Others were advancing a fringe theory that it would be worth the human cost to pursue herd immunity before a vaccine arrives.
Still others claimed that the increase in cases was due only to the greater testing that is being done.
In response to DeWine’s admonition that Ohioans “pay attention and get serious” about the spike, one skeptic seemed to need the most grisly proof before being convinced that the pandemic was real.
“Where are all the dead bodies, the mass burials, the pages upon pages of obituaries and the endless funeral processions?” #Trumpster tweeted. “I’m just not seeing it or believing it governor.”
The poster’s Twitter handle might have provided a clue as to the source of all the skepticism.
Asked about some of the myths being posted as fact, DeWine took particular exception to the claim that coronavirus cases are only increasing because there’s more testing.
“The whole idea that cases are going up solely because we are increasing testing is just nuts,” DeWine said, “It’s not right. The way you can tell it is look at our increase in (the rate of positive results.) Generally, if you go out and test a wider and wider group of people… and testing many people who don’t have symptoms, you would expect that the positivity rate would go down. That is not what has happened.”
Yet that claim has repeatedly been made by the man DeWine is supporting for president — Donald Trump. Most recently, Trump made it in a “60 Minutes” interview that’s scheduled to air on Sunday. In violation of his agreement with CBS, Trump released an unedited, 37-minute recording of the interview.
In the recording, Trump rarely allows the reporter, Leslie Stahl, to complete a sentence, but in a Tweet he claimed the opposite.
“Watch her constant interruptions and anger,” he wrote. “Compare my full, flowing and ‘magnificently brilliant” ‘answers to their ‘Q’s’.”
One of those “magnificently brilliant” statements was that the only reason covid case counts are spiking is due to increased testing. The same claim DeWine called “nuts.”
There was a similar gulf between Christie’s comments and those of Trump, his close political ally.
Christie described his diligent mask wearing, social distancing and hand washing. And then, for the first time in seven months, he skipped those precautions when he went to the White House to help Trump prepare for the first presidential debate with Democratic nominee Joe Biden.
“I walked through the gates and found out that I had tested negative at the White House Medical Unit, I took my mask off and I left it off, but only for the time I was inside those gates,” Christie said.
He later added, “I made a huge mistake by taking that mask off and I hope it’s something no other Americans have to go through.”
Jake Zuckerman is a statehouse reporter. He spent three years chronicling the West Virginia Legislature for The Charleston Gazette-Mail after covering cops and courts for The Northern Virginia Daily.
It started with a funeral.
Tina Maharath, a Democratic state senator from Canal Winchester, attended a wake Aug. 9 after her brother-in-law’s funeral, who died of non-COVID-19 illness.
Two of his family members, who Maharath said tested positive for COVID-19, came to the wake. Maharath described them as skeptical of the gravity of the COVID-19 pandemic.
“Slowly, one by one, we started getting the phone calls from each one of our family members,” she said in an interview.
Maharath comes from a big family — common, she said, among Laotians. Her husband has 19 siblings, she has 16. The new coronavirus, which causes COVID-19, left from the wake to invade 11 different family households, infecting 33 family members including a 9-month-old baby.
As of Thursday, two have died: Maharath’s 44-year-old sister-in-law, who had been battling brain cancer for a year, and her sister-in-law’s father-in-law.
Five family members were hospitalized, including one who Maharath said is likely to die soon from COVID-19. The five people hospitalized are between 34- and 76-years old. They were hospitalized anywhere from two to six weeks. Mahrath’s sister-in-law was ventilated for three weeks.
All five had underlying health conditions like asthma, high blood pressure and diabetes, all common conditions in Ohio.
The familial outbreak, Maharath said, is hopefully over. But uncertainty over longevity of symptoms or long term damage is frightening.
“We’re concerned because of the five people who were hospitalized, they still have lingering symptoms too, and another sister-in-law who was pregnant, she has lingering symptoms too,” Maharath said. “I don’t have underlying conditions, I’m not pregnant. So why do I have symptoms?”
Patient groups, calling themselves “long haulers,” have insisted they’ve been experiencing COVID-19 symptoms for month. The CDC has found COVID-19 can result in prolonged illness, even among younger and healthier adults.
Six weeks out from the positive test result, Maharath said she still feels COVID-19’s symptoms. She said she feels dehydrated, experiences coughing spells, and headaches.
Her lungs, she said, take most the heat.
“I just feel weak,” she said. “My lungs feel like something is just punching them. Randomly, it feels like something is just stabbing my lungs.”
Nearly 148,000 Ohioans have contracted COVID-19 according to state data, which officials believe to be an undercount. At least 4,715 have died.
Maharath’s diagnosis drew headlines in August. On Wednesday, however, Maharath shared the story of the outbreak through her family in a floor speech opposing Senate Bill 311.
The legislation, which Senate Republicans passed, would forbid the Ohio Department of Health from issuing anything like the stay-at-home order it issued in March, which closed “non-essential” businesses in an effort to slow the spread of the recently-detected coronavirus.
However, a COVID-19 diagnosis did not prove to be a proxy vote against the legislation.
Sen. Bob Peterson, R-Washington C.H., who contracted the disease earlier this month, voted in favor.
Sen. Frank Hoagland, R-Adena, did as well. He contracted a mild case of the disease in August. According to a Herald Star report, Hoagland’s wife was hospitalized with the disease as well. Both his wife’s parents reportedly died from COVID-19.
With what they hope to be the worst of the outbreak behind them, Maharath said her family is planning funerals for the deceased. They plan stricter social distancing and mask requirements.
The Home Energy Assistance Summer Crisis Program provides a one-time benefit to eligible Ohioans with cooling assistance during the summer months. The program runs from July 1 to September 30.
The focus of the Summer Crisis Program is to provide assistance with electric utility bills, central air conditioning repairs, and air conditioning unit and/or fan purchases.
Households with a household member who is either 60 years of age and older, has been diagnosed with COVID-19, or has a certified medical condition, and households who have a disconnect notice, have been shut off, or are trying to establish new electric service may be eligible for assistance.
Ohioans enrolled in the Percentage of Income Payment Plan Plus (PIPP) Program are eligible for assistance towards their default PIPP payment, first PIPP payment, central air conditioning repairs, or may receive an air conditioning unit and/or fan.
Who is Eligible for the Summer Crisis Program?
Ohioans with a household income at or below 175 percent of the federal poverty guidelines and have a member of the household who is at least 60 years old, has been diagnosed with COVID-19, or can provide physician documentation that cooling assistance is needed for a household member’s health, or households who have a disconnect notice, have been shut off, or are trying to establish new electric service.
Size of Household
Total Household Income 12 Months
1
up to $22,330
2
up to $30,170
3
up to $38,010
4
up to $45,850
5
up to $53,690
6
up to $61,530
7
up to $69,370
8
up to $77,210
For households with more than eight members, add $7,840 for each individual.
How do I apply for the Summer Crisis Program?
You can begin your application online at energyhelp.ohio.gov but will need to set up an appointment with your local Energy Assistance Provider in order to complete the application.
When you apply, you will need to complete the Energy Assistance Application (English or Spanish) and submit copies of the following documents.
copies of your most recent utility bills
a list of all household members (include birth dates and Social Security numbers) and proof of income for everyone in the household over 18 years old for the last 30 days for each member (12 months preferred)
proof of citizenship or legal residency for all household members
proof of medical condition verified by a licensed physician or registered nurse practitioner
You will need to include: proof of income for the past 30 days and 12 months for each member, a copy of your recent fuel/utility bill, proof of medical condition signed by a doctor or nurse practitioner, and a list of all household members (including Social Security Numbers).
Contact your local Energy Assistance Provider for a list of all required documents. Depending on your income type, additional forms may be required. Samples of the additional forms can be found by clicking here.
Frequently Asked Questions
How often can I apply for a HEAP Summer Crisis benefit?
You can apply for assistance through the HEAP Summer Crisis Program once a year.
What if I live in Federally Subsidized Housing?
Families who live in federally subsidized housing are not eligible unless the electric bill is in their name or they have verification that they are responsible for portion of the electric bill.
How do you define household income?
Household income is defined as the total annual gross income before taxes (minus exclusions) of all household members, except earned income of dependent minors under 18 years of age. All income and allowed exclusions must be documented for household members 18 years of age and older regardless of relationship to the primary applicant. Heads of households and spouses may never be considered minors. Gross household income includes wages, interest, dividends, annuities, and pensions.
Included (Countable) Household Income
Active Military Pay (Basic pay)
Adoption Assistance
Alimony
Annuity
Black Lung
Capital Gains – Proceeds from sale of property, home and stock
Cash Withdraws from Individual Retirement Accounts (IRA), Annuities, or other investments
Commissions
Company Disability
Disability Assistance (DA)
Estate and Trust Settlements – minus attorney fees – (one-time payment or lump sum)
Farm Income
Garnished Wages, including Bankruptcy/Chapter 13
Grants/Training Stipends – living expenses only
Immigrant Relocation Allowance
Interest earned from Savings Accounts
Legal Settlements
Lump Sum Distribution
Odd Jobs
Ohio Electronic Childcare (Ohio ECC) – Provider Income
Ohio Works First
Pensions – Government/Veterans/Private Industry
Rental Income earned from rental property
Seasonal Employment Income
Self-Employment Income
Social Security, Supplemental Security Income (SSI) Social Security Disability (SSDI) (Excluding Medicare Deductions)
Strike Benefits
Temporary Assistance to Needy Families (TANF)/General Assistance (GA)
Unearned income paid to or on the behalf of minors
Unemployment Benefits
Utility Allowances (as discretionary income)
Veteran’s Administration Benefits
Wages/Tips
Widows/Widower’s Benefits
Workers’ Compensation
Excluded Household Income
Adoption Assistance
Agent Orange Compensation/Benefit
Assets from bank withdrawals (90-day rule)
Attorney’s fees for Estate & Trust Settlements
Census Wages
Child Support Paid Out
Child Support Received
Education Assistance
FEMA Cash Payments
Food Assistance Benefit – Food Stamps, SNAP, etc. (cash or equivalent)
Funds/training stipends designated for specific purposes (i.e., educational Grants/Training stipends for tuition and/or books only-not living expenses)
Gifts
Handicapped Income – self-sufficiency programs (example: work expenses for the blind)
Health Care Spending Accounts – non-taxable health care spending accounts are allowable
Health Insurance Premiums (dental, vision, health and supplemental insurance)
Income earned by dependent minors less than 18 years of age
Jury Duty
Loans from individuals or institutions requiring repayment of either principle or principal and interest*
Medicaid spend-down
Medicare Part D (prescription premium)
Medicare Payments
Military Allowances for Subsistence, Housing, Family Separation, etc.
Ohio Waiver Program
Prevention, Retention, & Contingency (PRC) – assistance to attempt to divert families from long term financial dependency
Proceeds from reverse mortgages
Reimbursement for work expenses
SS/SSI and SSDI overpayments
Stipend for Foster Care
Tax refunds and rebates
Title III Disaster Relief Emergency Assistance Program (DREAP)
Title V Wages/Senior Community Employment Programs (SCEP) – Older Americans’ Act (Public Law 100-175) Experience Works (formerly Green Thumb), Foster Grandparents Program, Mature Services
Volunteers in Service to America (Vista) or other AmeriCorps Stipends
Work Allowances (i.e., Learning Earning and Parenting [LEAP])
Work programs for people with disabilities
I have applied for HEAP, but I may be disconnected from my utility service. Can I apply for Summer Crisis assistance?
Yes, you can apply for the Summer Crisis Program. Contact your local Energy Assistance Provider to apply.
Who can I call with questions about the Home Energy Assistance Summer Crisis Program?
You can call the Ohio Development Services Agency’s hotline (800) 282-0880 or your local Energy Assistance Provider by clicking here.
Other Programs
If you’re having trouble managing your home energy costs, there is help. Below is a list of programs that can help you manage your utility bills and improve your home’s energy efficiency. You also can find a list of local Energy Assistance Providers and a copy of the program application.
You also can apply for assistance online. Visit energyhelp.ohio.gov to complete your application.
This article provided to Loveland Magazine was edited by David Miller and is by by Eye on Ohio, the nonprofit, nonpartisan Ohio Center for Journalism. Please join their free mailing list as this helps us provide more public service reporting.
In early March, just as Ohioans were learning about the first cases of novel coronavirus in the state, Anna Bondar’s grandfather fell at his Cleveland home.
Luckily, the 92-year old, who lives with dementia, wasn’t injured badly.
The tight-knit family started to discuss the possibility of a nursing home, though they had serious reservations.
Their tough choice was made even more difficult by mounting fears about the coronavirus. In nearly four months, COVID-19 has infected more than 31,191 people statewide and has proven particularly deadly for residents of long-term care facilities in Ohio.
Seventy percent of the reported deaths in Ohio due to COVID-19 complications have been in long-term care facilities, which is among the highest in the country.
Nationally the portion of COVID-19-related deaths in long-term care facilities has hovered just over 40%, though the amount of testing done in nursing homes varies significantly by state.
Every day, families like Bondar’s are making what can feel like an impossible choice – whether to send a loved one to a nursing home where they will receive around-the-clock specialized care but face a greater risk of contracting COVID-19, or to care for that person at home where risk of transmission is lower but providing care can be more challenging.
Even before the pandemic, sorting through the myriad of quality ratings and measures was daunting enough. Then, COVID-19 deaths started to soar.
Now, families and seniors agonize over what could be life or death choice using confusing numbers on infection “hotspots” and without the ability to visit nursing homes to observe how the staff cares for residents – which is the number one recommendation of most advocates.
Dr. Amy Acton, director of the Department of Health
State officials, including Dr. Amy Acton, the former director of the Department of Health, have emphasized that “congregate” settings like nursing homes are at highest risk of infection. Staff, who often travel between facilities, need to be in close contact with residents to provide care. And residents, who are primarily older and have multiple medical conditions, are more susceptible to COVID-19-related complications.
“All of this makes it high risk. At the same time, it’s really necessary for many patients to be there,” said Dr. Steven Schwartz, a geriatric physician at the Cleveland Clinic who travels to nursing homes as part of the Clinic’s Center for Connected Care.
Ohio National Guardmembers will begin testing all staff members and any residents who likely were exposed to COVID-19 in the state’s nursing homes, Gov. Mike DeWine announced May 27. What are being called Congregate Care Unified Response Teams will focus on facilities where confirmed or assumed positive cases are reported in hopes of reducing the number of COVID-19 cases and deaths in Ohio’s nursing homes, which as of May 27 was 5,324 resident cases and more than 1,442 deaths.
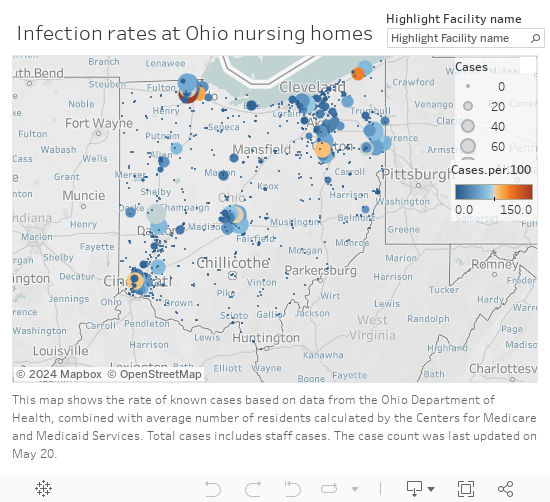
Infection rates in Ohio Nursing Homes
Making an educated decision
Last month, state officials began to release the numbers of reported infections and deaths in long-term care facilities, which include nursing homes, rehabilitation centers, and assisted living centers.
But it’s unclear how much the numbers – which are reported weekly and are also tracked cumulatively – matter for families currently trying to choose a facility.
The state, on its coronavirus website, says the infection and death numbers shouldn’t replace a thoughtful conversation with a nursing facility about infection control practices and that “residents and family members should understand that the presence of COVID-19 at a facility is [in] no way an indicator of a facility that isn’t following proper procedures.”
Yet many in the health care industry say infection information should be considered, along with other factors, when deciding which site to choose.
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck.”
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck,” said Dr. James Campbell, department chair of geriatric medicine at MetroHealth.
The infection information provided by the state can be useful, for instance, if a family is choosing between two similar facilities, said Nate Cyrill, a Long Term Care Ombudsman for Cuyahoga, Geauga, Lake, Lorain and Medina counties.
Since information on the virus changes rapidly, most families still rely on the quality measures that were available before COVID-19, including existing state and federal online guides Cyril said.
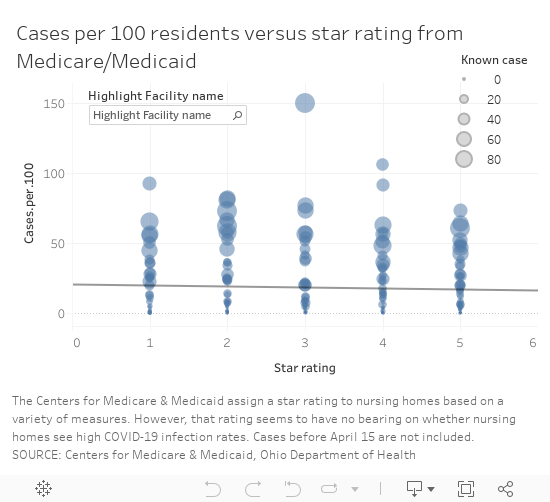
One of the commonly-used ranking systems, maintained by the Centers for Medicare and Medicaid Services, assigns ratings – from 1 to 5 “stars” – to facilities based on performance on quality measures, staffing and inspections.
The number of “stars” Ohio’s nursing homes received, however, does not appear to have a correlation to the number of infections reported to the state, based on a comparison of the publicly available information. The analysis did not include assisted living facilities.
Cases vs. Star rating
“You want to look for a nursing home that’s four of five stars preferably but even that doesn’t tell you the whole story,” Steven Schwartz said.
There are numerous 1-star rated facilities that have reported few infections, like Whetstone Gardens and Care Center in Columbus, which has reported 9 cases or 8 per 100 residents.
Salem North Healthcare Center
Salem North Healthcare Center in northern Columbiana County had 51 patients test positive for the virus as of May 20, as well as five staff, according to the state. It is rated a 5-star facility, the highest rating from CMS.
It’s one of four 5-star facilities with an infection rate over 50 casesper 100 residents, based on Medicare’s calculation of each facility’s average number of residents. (The rate does not include infections among staff because the number of staff in each facility was not available.)
Since April, the focus on high numbers of reported infections, often referred to as clusters, in long-term care facilities has intensified. In some cases, those numbers are a reflection of the level of testing, said Fred Stratmann, general counsel and chief compliance officer for CommuniCare Health Services. It doesn’t mean all of the residents with a positive test had symptoms of COVID-19. The state infection numbers also don’t show the residents who have recovered from the virus, he said.
CommuniCare, which operates close to 90 health care facilities in seven states has been proactive about testing, Stratmann said. When COVID-19 cases started to appear at the North Salem facility, the company enlisted the state’s “strike team” to proactively test all of the residents. It has since re-tested all of the residents who were initially negative and purchased 3,000 testing kits to supplement what the state could provide.
“We wanted to be certain of the extent of COVID in this center in order to be able to properly treat it and to fight back against it,” Stratmann said. The facility does that by isolating any COVID-19-postive patients in a separate unit with its own dedicated staff and by admitting new residents to an observation unit for 14 days to make sure they have no symptoms of infection, he said.
Restrictions on visits make choices harder
The most effective way to scout out a facility typically is to visit it, preferably unannounced, said Dr. James Campbell, department chair of geriatric medicine at MetroHealth. However, because visitors aren’t permitted in nursing homes right now, the next best thing is to ask detailed questions about care, any COVID-19 cases and infection control measures, he said.
Campbell also suggested turning to hospital staff, who work with nursing homes regularly, for advice. Social workers can place five people in a week, while most individuals face that decision, at most, only a few times in their lives, he said.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
The agency, along with other similar independent agencies across the state, investigates complaints in long-term care, skilled nursing, group homes and rehabilitation facilities and can share what are called “verified complaints” that aren’t otherwise available publicly.
Most of the complaints investigated in relation to COVID-19, Cyrill said, have been related to visitation or the ability of families to get information on a loved one’s condition.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
Under normal circumstances, an ombudsperson would go to the facility and talk to patients and could do so without announcing the visit in advance. Since visits are restricted for infection control reasons, they have to work through staff to speak to residents or to ask questions, which isn’t optimal. And they aren’t able to make direct observations.
“It makes our job much more challenging,” Cyrill said.
At the North Salem facility, which has had about a dozen new residents admitted or transfered from other facilities, the staff has given “virtual tours” over the phone to family members or prospective residents who were in the hospital, Stratmann said. The company also invested in technology that won’t replace face-to-face visits but enables more family contact and the ability and for staff to help keep residents’ spirits up by making videos of activities, like dancing and singing, to keep them connected with the local community.
In addition, Stratmann said they walk families through the infection control procedures and share techniques they have implemented to improve health outcomes for patients with COVID-19 including, when appropriate:
Treating residents with anticoagulant medications to reduce the risk of blood clots and strokes, which has been a factor in some COVID-19-related fatalities.
Practicing “proning” or positioning residents, while awake, flat on their belly and chest to reduce the buildup of fluid in lung tissue and reduce the risk of Acute Respiratory Distress Syndrome, which has been associated with many COVID-19 fatalities.
The idea of putting their beloved grandfather in a nursing home was gut-wrenching
Choosing home
For Bondar’s family, the idea of putting their beloved grandfather in a nursing home was gut-wrenching, especially as visitation was curtailed to limit the virus’ spread. He speaks Russian, his native language, and would not have been able to communicate well with the staff caring for him.
“It felt like admitting him [to a facility] would be like saying goodbye,” Bondar said. “Like leaving him to die.”
Bondar’s family ultimately decided to care for her grandfather at home, in his Mayfield Heights senior highrise, where they could limit his exposure to the virus.
Before his fall, an aide visited for about eight hours a week. After the Ohio’s “stay at home” order was put in place March 23, Bondar and her mother were able to work from home and pitch in with care.
The advice of the Clinic’s Steven Schwartz led them to a hospice program, which helped the family find additional aides, including one who speaks Russian, as well as a hospital bed for safer sleeping and a wheelchair.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
“We’ll do this as long as we can manage it,” Bondar said.
Anecdotally, it is a choice more families are making: the decision to use home care or even pull family members out of nursing homes out of fear or because they miss them and can’t visit, Steven Schwartz said.
“Sometimes it’s appropriate. But sometimes, even given everything, it may be safer to have your family member there to get stronger and get the necessary care,” said Steven Schwartz. “I would really try to balance the benefit of going to a nursing home versus the risk.”
Patients with dementia or Alzehimer’s may be unsafe going back home.
Patients with dementia or Alzehimer’s may be unsafe going back home, he said, and families may need to decide if a nursing home really is the safer place.
One of the first orders Ohio put in place to prevent the spread of COVID-19 was to halt in-person visitation in more than 900 nursing and long-term care facilities. The state is not yet ready to lift those restrictions and resume visits in those settings, Gov. Mike DeWine said, but on June 8 will start allowing outdoor visits at assisted living facilities care centers for individuals with disabilities.
“We are not to nursing homes yet and I know that causes anguish for a lot of people who are watching this but we’re trying to do this so that we don’t increase the COVID inside the nursing homes or the assisted living or the immediate care facilities,” DeWine said during a May 28 briefing.
Decisions made harder
Figuring out what kind of care might be best for a patient has become more challenging, too.
Previously, nurses and social workers would visit clients in their homes to assess how they functioned – whether they could independently bathe, cook and grocery shop, said Theresa Foster, a nurse and licensed social worker at Western Reserve Area Office on Aging.
They relied on conversations with clients and family and also observations of the environment in the home and possible risks, said Foster, who runs the agency’s resource center.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Now, those assessments are done by phone and can be done successfully, but it is more difficult, Foster said.
At UH’s hospitals, medical staff use a scoring system to determine the best place for a patient being discharged, said Dr. Sean Cannone, UH’s medical director for population health.
Patients are assessed on their ability to perform daily tasks and on their cognitive abilities.
“We’re trying as much as we can to get patients home if at all possible,” he said. The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
“We want to respond to what people really want for their own care,” Cannone said.
The shift started before COVID-19 cases surfaced but has accelerated as more families worry about potential exposure to the virus in congregate living situations.
As technology has advanced, the capabilities of what can be done in a patient’s home has also increased. In March, UH introduced a new patient management system, Massimo SafetyNet, for remote monitoring.
When patients are released from the emergency room or from a COVID-19 floor, providers now put a bluetooth sensor on their wrist — it looks like an Apple Watch — that streams data about a patient’s vitals to a central monitoring center, said Jonathan Sague, UH’s vice president of clinical operations. That way, providers can make sure a patient is safe at home.
Douglas Beach is the chief executive officer at Western Reserve Area Office on Aging
Douglas Beach, chief executive officer at Western Reserve Area Office on Aging, has had firsthand experience weighing care decisions amid COVID-19 worries. His mother is rehabilitating in a nursing home after a six-week hospital stay related to a heart condition.
Not being able to visit her in the hospital or the facility has been hard, Beach said. He and his brother, who is a doctor, had to make all of the arrangements by phone, including figuring the best way to transport her that would have the lowest risk of exposure to the virus.
“Home and community-based services is what I do,” Beach said. Part of his mission is to advocate for the setting that allows for any person, whether they are older adults or live with a disability, to be as independent as possible .
But for his mother, a nursing facility was the right choice because she needed 24-hour care that her family could not provide at home.
Beach said nursing homes have had to deal with an unprecedented set of circumstances: a new virus, initial unknowns about transmission and populations at extremely high risk for complications.
Nursing homes will continue to play a vital role and will remain the best option for people who need more care than can be safely provided at home, Beach said.
For the more than 9,500 clients his agency serves in Cuyahoga, Geauga, Lake, Lorain and Medina counties, delivering care at home, with health aides, nurses and community and family supports, has proven a low risk. As of mid-May only 35 clients had tested positive for the virus, he said. That is roughly 0.3% of clients, though not all clients are tested.
Managing COVID-19
Cuyahoga County nursing homes have been paired with one of the area’s three largest hospital systems during the pandemic, Campbell said. The hospitals help the facilities both prepare for and respond to COVID-19 cases.
“The goal is when you have one patient in a nursing home with COVID is to make sure you don’t end up with 30 patients with COVID,” Campbell said.
UH developed what is being called a playbook for local nursing homes. The playbook gives facilities a plan for how to respond if there’s a COVID-19 outbreak on-site, said Sague, who works as a firefighter and medic on the weekends.
“It can be pretty startling and pretty alarming if they’re not ready for it,” Sague said.
The playbook gives guidelines on screening, triaging, determining exposure, testing and isolating those who test positive, as well as how to get personal protective equipment, increase staffing and to eventually reopen safely, Sague said.
Once a case is identified at a facility, what is known as an intercept team is dispatched — either virtually or in person — to help a nursing home handle it, he said.
Patrick Schwartz, director of strategic communications for LeadingAge Ohio, a long-term care trade association, said access to testing and safety equipment has been a consistent problem for Ohio’s nursing homes.
But in the past month or so, the state has made “a definite shift” and started prioritizing testing at nursing homes, which is helping, he said.
Patrick Schwartz said he hoped the expanded testing would enable facilities to test their entire population— of residents and staff — so they can better limit the spread of the virus.
Throughout Ohio, populations that have received mass testing — health care workers, first responders, those incarcerated and those in nursing homes — have had higher numbers of positive cases. Many people with COVID-19 are asymptomatic, so it is unknown if they have the virus until they are tested.
“Since this pandemic first reared its head, it was clear to long-term care providers that the front lines would be in long-term care,” Patrick Schwartz said. The populations at those congregate living facilities, many of whom are older and have multiple medical conditions, are among the most vulnerable for complications from COVID-19, he said.
In Cuyahoga County, and elsewhere, local health departments have deployed limited testing resources to nursing homes quickly in hopes of limiting spread in and between facilities and given guidance to homes about how to isolate patients and trace exposures between facilities to limit the spread of infection.
Cuyahoga County Health Commissioner Terry Allan said nursing homes try to guard against outbreaks but have varying degrees of resources. The assistance from the National Guard will allow more residents and staff at facilities in Northeast Ohio to be tested, he said.
Support for this project was provided by the Center for Community Solutions.
Questions to ask:
How can family members stay in touch with residents while visiting is restricted?
Does staff facilitate video visits? Is window visiting allowed?
How often will the facility provide updates on a resident’s condition?
How much COVID-19 testing is being done? Is the facility proactively testing patients or only those with symptoms?
Are private rooms available?
Do staffing ratios allow for residents to be taken outside?
Are residents currently restricted to rooms?
Are separate units and staffs used for COVID-19-positive patients and COVID-19-negative patients?
How does the facility work to limit COVID-19 complications?
Ohioans who are eligible for the Supplemental Nutrition Assistance Program (SNAP) can now use their Ohio Direction cards to purchase food online through Walmart and Amazon, the Ohio Department of Job and Family Services (ODJFS) has announced.
“We know many Ohioans are struggling and that food purchasing has been a challenge for many, especially older Ohioans and those with limited access to transportation,” said ODJFS Director Kimberly Hall. “We hope online purchasing gives individuals more options and makes it easier for them to both stay safe and eat nutritiously.”
Previously, Ohio SNAP recipients could order groceries online at Giant Eagle, Walmart and some Kroger stores, but they had to pay inside the stores or at curbside. After receiving federal approval, ODJFS successfully tested online purchasing with Walmart and Amazon. While Ohio SNAP recipients can order food online from a variety of retailers, only Walmart and Amazon allow online purchasing with EBT cards. Individuals may choose to have groceries delivered, but federal rules still prohibit using SNAP benefits to pay for any delivery charges.
Qualify for SNAP
Individuals may qualify for SNAP if their household’s gross monthly income is at or under 130% of the federal poverty guidelines. Ohioans can apply at benefits.ohio.gov. Benefits can be used to buy most food products, with the exception of alcoholic beverages, vitamins and/or medicines, and hot food
made to be eaten immediately, including prepared food from grocery stores and restaurants.
ODJFS has provided additional assistance to SNAP recipients during the pandemic:
Began issuing Pandemic EBT benefits for children who normally receive free or reduced price meals at school.
Issued supplemental SNAP payments to qualifying households in March, April and May and is preparing to issue them again in June.
Waived administrative verifications normally required at food banks, to streamline the process and limit person-to-person contact.
Extended SNAP recertification periods for March, April, May and June by six months.
Media Statement: Ballot Access July 02, 2018, 14:00 EDT
For further information, contact:
Harold Thomas, LPO Chair harold.thomas@lpo.org (614) 581-6832
David Jackson, Communication Director david.jackson@lpo.org
(614) 560-1237
July 2, The Libertarian Party of Ohio filed petitions containing 102,762 signatures with the Secretary of State to regain ballot access taken away from the citizens of Ohio four years ago because of Republican Party politics
They intended to destroy the Libertarian Party in Ohio.
But liberty and choice persevered. We have more volunteers and more enthusiasm than ever. Putting us through the political tricks has made us stronger.
We are stronger knowing that 102,762 voters are signed their names to give Ohio more and better choices to address our economic and social issues. Ohioans want solutions, and sense that the way forward might lie in less government, instead of more. These petitions came from all 88 counties showing support from every part of this state. We are building from a broad base of voters from every economic level; all racial backgrounds; all faiths, and all sexual orientations, helping the ever-expanding diversity of our party.
We know that establishment trickery will not end here. We have attorneys armed with the Constitutions of the United States and the State of Ohio. We know of some recent federal court decisions in other states that have made challenger party ballot access easier, not more difficult. Our attorneys are ready to deal with any obstacles they throw our way. However, we seek no fight, just open dialog and new ideas.
The establishment parties will try to convince you that we are “Republicans-lite” or agroup of spoilers whose primary purpose is to throw elections one way or the other. Some will even try to make you believe that we are anarchists bent on social chaos. Don’t believe them. The Libertarian Party has members all around you and is the only party with a consistent philosophy and platform — one we have followed, faithfully, since our inception nearly 50 years ago. Our philosophy is based on this Golden Rule, which call it the “non-aggression principle.” No one, including government, has theright to use force to promote a political or social agenda. Government aggression should only be used to protect our lives, our property, and our rights from those who would kill, rob, and cheat us.
Libertarians believe that government exists for one purpose, which Thomas Jefferson made clear in the Declaration of Independence. We are endowed with certain inalienable rights: life, liberty, and the pursuit of happiness, and that the purpose of government is to secure these rights. The framers of the Constitution reinforced the Declaration when they wrote in the Preamble that government’s purpose is to “establish justice, insure domestic tranquility, provide for the common defense, and secure the blessings of liberty to ourselves and our posterity.
It is a government for adults who can make their own decisions, build their own careers, and have values they want to pass on to their children. Our political system is broken because we have forgotten that. We have allowed our politicians – at all levels –to behave like children, focusing on trivial issues, fighting the cultural wars of past generations, and doling out favors to their largest contributors.
It’s time to stop this madness. It’s time to stop bickering and to start negotiating real solutions for Ohio. It’s time to engage in the politics of hope instead of the politics of fear. In this spirit, we will cooperate with members of the establishment parties and the Green Party on issues of mutual interest. Together, we can form policies designed to benefit all of us.
On Saturday, July 14, we will introduce our slate of candidates to you and the people of Ohio. You will find that they represent a new generation of leadership with fresh ideas and a new perspective on governing our state.
I invite you and all Ohioans to embrace the Libertarian Party and its candidates as we represent a true choice. We will not only show how to fix a broken system, and make it robust enough to secure the blessings of Liberty for ourselves and our posterity.
![[Commentary] Suicide is on the rise in Ohio](https://lovelandmagazine.com/wp-content/uploads/2024/02/988-suicide-prevention-2-1024x791-1-700x541-1.jpg)










 Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services. 



 “We know many Ohioans are struggling and that food purchasing has been a challenge for many, especially older Ohioans and those with limited access to transportation,” said ODJFS Director Kimberly Hall. “We hope online purchasing gives individuals more options and makes it easier for them to both stay safe and eat nutritiously.”
“We know many Ohioans are struggling and that food purchasing has been a challenge for many, especially older Ohioans and those with limited access to transportation,” said ODJFS Director Kimberly Hall. “We hope online purchasing gives individuals more options and makes it easier for them to both stay safe and eat nutritiously.” can be used to buy most food products, with the exception of alcoholic beverages, vitamins and/or medicines, and hot food
can be used to buy most food products, with the exception of alcoholic beverages, vitamins and/or medicines, and hot food

