If you have household or social contact with someone at high risk for getting very sick, consider self-testing to detect infection before contact, and consider wearing a high-quality mask when indoors with them
HIGH
When the COVID-19 Community Level is High:
Wear a high-quality mask or respirator.
If you are at high risk of getting very sick, consider avoiding non-essential indoor activities in public where you could be exposed.
Community-Level Prevention Strategies
LOW, MEDIUM, AND HIGH
At all COVID-19 Community Levels:
Promote equitable access to vaccination, testing, masks and respirators, treatment and prevention medications, community outreach, and support services.
Ensure access to testing, including through point-of-care and at-home tests for all people.
Background: On 8/12/22 new guidance for school came out from both the CDC and ODH (ODH memo 8/12/22 updated COVID guidance. Here is the information that will help you here in LCSD:
Positive cases
5+5 (5 days of isolation followed by 5 days of masking) plan as outlined by CDC/ ODH (Ohio Dept of Health). This is calculated from the first day of symptoms or positive test which is considered day 0. If a student is not ready to come back after 5 days (your child needs to be fever free for 24 hours without fever-reducing medications and symptoms improving), parents would call to tell attendance daily if their child is not ready to return. These are considered non-absence days
Masking is not optional. If you have been positive, you will need to mask for 5 days after being in isolation for 5 days.
There are no online learning links available.
Extracurriculars- able to participate as long as able to mask. Removing mask is not an option
District nurses (DN) make the follow up phone calls to parents once we are notified of a positive case.
Close contacts/ exposures
Quarantine is no longer recommended for people who are exposed to COVID-19 except in certain high-risk congregate settings (not schools). Instead of quarantining if you were exposed to COVID 19, it is recommended that you wear a high quality mask for 10 days and get tested on day 5. For extracurriculars, they can mask as able to.
If your child has symptoms or develops symptoms, parents should keep them home and connect with their healthcare provider for further guidance and/ or covid testing. Testing on the same day as symptoms is now recommended.
Parents should tell the attendance person the absence is covid related.
If a student has a pending test and they have symptoms, we support keeping their child home until test results. If asymptomatic, they can be at school masked during that time
We will no longer be monitoring vaccination status
These days are excused absences, but we will continue to monitor
3 . Testing
Any testing except antibody testing is acceptable.
Recommend testing day five per HCPH guidelines for exposures, but not required
4. Vaccines
We encourage everyone to talk to their health care provider for themselves and their children regarding getting vaccinated for COVID. It is the best way to address COVID going forward. Students over 5 are now eligible for the first booster vaccine
LCSD will continue to focus on “The Bundle”- handwashing, cleaning, distancing as needed/ able to, and masking when appropriate/ optional choice. Our entire staff is committed to keeping our students safe and healthy. We need your support by you doing the wellness checks daily with your child(ren) and keeping them home if they are sick. Thanks for partnering with us- we can do anything together!!
Some of Ohio’s colleges and universities have begun moving students in, but the navigation of a school year amid a pandemic is still a balancing act.
For Miami University, classes began this week, with all undergraduate courses online or remote. The plan is to keep it that way until at least Sept. 21, according to the plan posted to the school’s website.
“When we began planning last spring, we had hoped that the COVID-19 pandemic would be in significant decline before classes were scheduled to begin,” Miami president Greg Crawford told students. “Instead, cases are rising in many states. With 40% of our Oxford students coming from outside Ohio, we’ve been monitoring the situation closely.”
Those that are on campus are required to wear masks, and as students come back, they can be reported to the Office of Community Standards if they repeatedly refuse to comply with an instructor’s direction to use a mask or face covering.
Mask requirements are the norm among Ohio’s public colleges and universities, as are 14-day quarantines for students coming from states considered COVID-19 hotspots.
Also the norm this school year are phased reopenings, like those at The Ohio State University, Ohio University, Kent State University, Shawnee State University, Cleveland State University, and the University of Cincinnati.
The first move-in dates for UC, Aug. 14 and 15 were considered “drop-off only,” meaning students could bring their stuff to campus, but then had to return home until the 16th.
Another regular part of public colleges’ and universities’ schedules is a return to at least some form of in-person class instruction that ends after Thanksgiving break. The last two weeks, including final exams, will be taken remotely at OSU, Central State University, UC, KSU and Wright State University, among others.
Kent State and the University of Toledo have eliminated their fall break to allow students to receive a full semester despite adjusted opening dates.
Toledo said they adjusted their Fall semester “based on the possibility of having a second wave of COVID-19 in late fall,” taking into account CDC data on the pandemic and state recommendations for higher education.
Bowling Green State University went so far as to cancel their Winter 2021 session and provide a $1,500 credit for the first 2,000 students who cancelled their housing assignment before the school year began this week.
“It is important you understand that we are HIGHLY encouraging you not to live on campus this fall,” information on the university’s COVID-19 plan page stated.
BGSU started their staggered move-in this week for those that had no other option than to take up residence, and are set to begin classes on Aug. 31. Students there will also be online only beginning Nov. 30.
OU phased in their reopening by allowing certain graduates and undergraduates “in a carefully selected set of academic programs” to begin their time on campus. Most students will begin remotely on Aug. 24, but students like third-year students in the College of Health Sciences and Professions’ nursing program and juniors and seniors in the Army Reserve Officer Training Corps (ROTC) are eligible to participate in the university’s first phase of schooling.
Universities throughout the state sticking with in-person instruction have instituted class-size reductions, along with “hybrid-remote” forms of teaching. Central State spelled out a “cohort attendance” model in its reopening plan, which would break large classes into groups, with the cohorts attending classes on alternating days. This model goes along with a 50% reduction in class sizes, something Wright State anticipates as part of its plan as well.
“At this time, the university conservatively estimates that one-third of classes will have in-person components while the majority of in-person classes will also deliver all content remotely to provide flexibility to students who are unable or do not feel comfortable returning to campus,” said Wright State president Susan Edwards in a letter to the university community.
Many of Ohio’s public higher education institutions have also created pledges for students connected to prevention of coronavirus, and in some cases can spur disciplinary action if not signed.
Testing and contact tracing for COVID-19 are a regular part of all public school plans, though the ways in which the testing is done vary from school to school.
The spring semester plan is still to be determined for most schools. The University of Akron plans to continue hybrid online and in-person instruction into the spring, but others are still watching the success of their fall semesters to plan for the future.
“Decisions are forthcoming,” stated the UC reopening plan.
Susan Tebben is an award-winning journalist with a decade of experience covering Ohio news, including courts and crime, Appalachian social issues, government, education, diversity and culture. She has worked for The Newark Advocate, The Glasgow Daily Times, The Athens Messenger, and WOUB Public Media. She has also had work featured on National Public Radio.
This article provided to Loveland Magazine was edited by David Miller and is by by Eye on Ohio, the nonprofit, nonpartisan Ohio Center for Journalism. Please join their free mailing list as this helps us provide more public service reporting.
In early March, just as Ohioans were learning about the first cases of novel coronavirus in the state, Anna Bondar’s grandfather fell at his Cleveland home.
Luckily, the 92-year old, who lives with dementia, wasn’t injured badly.
The tight-knit family started to discuss the possibility of a nursing home, though they had serious reservations.
Their tough choice was made even more difficult by mounting fears about the coronavirus. In nearly four months, COVID-19 has infected more than 31,191 people statewide and has proven particularly deadly for residents of long-term care facilities in Ohio.
Seventy percent of the reported deaths in Ohio due to COVID-19 complications have been in long-term care facilities, which is among the highest in the country.
Nationally the portion of COVID-19-related deaths in long-term care facilities has hovered just over 40%, though the amount of testing done in nursing homes varies significantly by state.
Every day, families like Bondar’s are making what can feel like an impossible choice – whether to send a loved one to a nursing home where they will receive around-the-clock specialized care but face a greater risk of contracting COVID-19, or to care for that person at home where risk of transmission is lower but providing care can be more challenging.
Even before the pandemic, sorting through the myriad of quality ratings and measures was daunting enough. Then, COVID-19 deaths started to soar.
Now, families and seniors agonize over what could be life or death choice using confusing numbers on infection “hotspots” and without the ability to visit nursing homes to observe how the staff cares for residents – which is the number one recommendation of most advocates.
Dr. Amy Acton, director of the Department of Health
State officials, including Dr. Amy Acton, the former director of the Department of Health, have emphasized that “congregate” settings like nursing homes are at highest risk of infection. Staff, who often travel between facilities, need to be in close contact with residents to provide care. And residents, who are primarily older and have multiple medical conditions, are more susceptible to COVID-19-related complications.
“All of this makes it high risk. At the same time, it’s really necessary for many patients to be there,” said Dr. Steven Schwartz, a geriatric physician at the Cleveland Clinic who travels to nursing homes as part of the Clinic’s Center for Connected Care.
Ohio National Guardmembers will begin testing all staff members and any residents who likely were exposed to COVID-19 in the state’s nursing homes, Gov. Mike DeWine announced May 27. What are being called Congregate Care Unified Response Teams will focus on facilities where confirmed or assumed positive cases are reported in hopes of reducing the number of COVID-19 cases and deaths in Ohio’s nursing homes, which as of May 27 was 5,324 resident cases and more than 1,442 deaths.
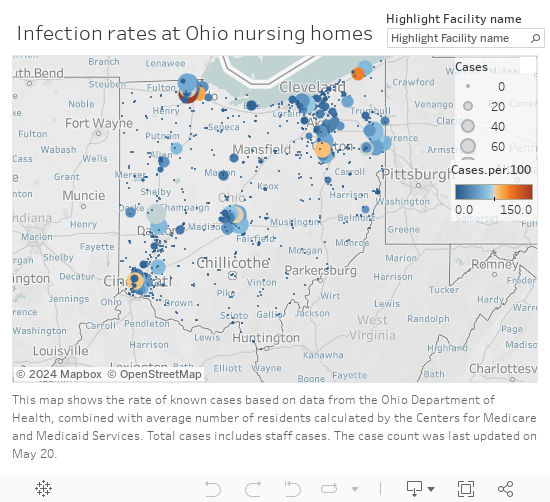
Infection rates in Ohio Nursing Homes
Making an educated decision
Last month, state officials began to release the numbers of reported infections and deaths in long-term care facilities, which include nursing homes, rehabilitation centers, and assisted living centers.
But it’s unclear how much the numbers – which are reported weekly and are also tracked cumulatively – matter for families currently trying to choose a facility.
The state, on its coronavirus website, says the infection and death numbers shouldn’t replace a thoughtful conversation with a nursing facility about infection control practices and that “residents and family members should understand that the presence of COVID-19 at a facility is [in] no way an indicator of a facility that isn’t following proper procedures.”
Yet many in the health care industry say infection information should be considered, along with other factors, when deciding which site to choose.
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck.”
“If you see a nursing home with a large outbreak, that’s something to worry about. If you see a nursing home with a small outbreak, I’m not sure it means anything but bad luck,” said Dr. James Campbell, department chair of geriatric medicine at MetroHealth.
The infection information provided by the state can be useful, for instance, if a family is choosing between two similar facilities, said Nate Cyrill, a Long Term Care Ombudsman for Cuyahoga, Geauga, Lake, Lorain and Medina counties.
Since information on the virus changes rapidly, most families still rely on the quality measures that were available before COVID-19, including existing state and federal online guides Cyril said.
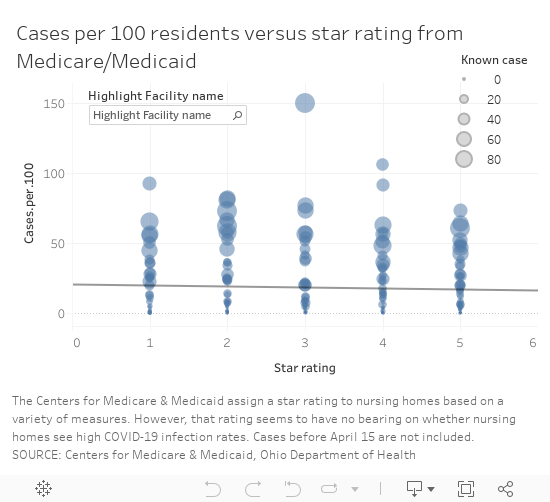
One of the commonly-used ranking systems, maintained by the Centers for Medicare and Medicaid Services, assigns ratings – from 1 to 5 “stars” – to facilities based on performance on quality measures, staffing and inspections.
The number of “stars” Ohio’s nursing homes received, however, does not appear to have a correlation to the number of infections reported to the state, based on a comparison of the publicly available information. The analysis did not include assisted living facilities.
Cases vs. Star rating
“You want to look for a nursing home that’s four of five stars preferably but even that doesn’t tell you the whole story,” Steven Schwartz said.
There are numerous 1-star rated facilities that have reported few infections, like Whetstone Gardens and Care Center in Columbus, which has reported 9 cases or 8 per 100 residents.
Salem North Healthcare Center
Salem North Healthcare Center in northern Columbiana County had 51 patients test positive for the virus as of May 20, as well as five staff, according to the state. It is rated a 5-star facility, the highest rating from CMS.
It’s one of four 5-star facilities with an infection rate over 50 casesper 100 residents, based on Medicare’s calculation of each facility’s average number of residents. (The rate does not include infections among staff because the number of staff in each facility was not available.)
Since April, the focus on high numbers of reported infections, often referred to as clusters, in long-term care facilities has intensified. In some cases, those numbers are a reflection of the level of testing, said Fred Stratmann, general counsel and chief compliance officer for CommuniCare Health Services. It doesn’t mean all of the residents with a positive test had symptoms of COVID-19. The state infection numbers also don’t show the residents who have recovered from the virus, he said.
CommuniCare, which operates close to 90 health care facilities in seven states has been proactive about testing, Stratmann said. When COVID-19 cases started to appear at the North Salem facility, the company enlisted the state’s “strike team” to proactively test all of the residents. It has since re-tested all of the residents who were initially negative and purchased 3,000 testing kits to supplement what the state could provide.
“We wanted to be certain of the extent of COVID in this center in order to be able to properly treat it and to fight back against it,” Stratmann said. The facility does that by isolating any COVID-19-postive patients in a separate unit with its own dedicated staff and by admitting new residents to an observation unit for 14 days to make sure they have no symptoms of infection, he said.
Restrictions on visits make choices harder
The most effective way to scout out a facility typically is to visit it, preferably unannounced, said Dr. James Campbell, department chair of geriatric medicine at MetroHealth. However, because visitors aren’t permitted in nursing homes right now, the next best thing is to ask detailed questions about care, any COVID-19 cases and infection control measures, he said.
Campbell also suggested turning to hospital staff, who work with nursing homes regularly, for advice. Social workers can place five people in a week, while most individuals face that decision, at most, only a few times in their lives, he said.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
Cyrill said his agency can also provide information that can’t be found online for families trying to choose between facilities.
The agency, along with other similar independent agencies across the state, investigates complaints in long-term care, skilled nursing, group homes and rehabilitation facilities and can share what are called “verified complaints” that aren’t otherwise available publicly.
Most of the complaints investigated in relation to COVID-19, Cyrill said, have been related to visitation or the ability of families to get information on a loved one’s condition.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
It’s been harder, though, for Cyrill and his colleagues to investigate complaints with COVID-19 restrictions in place.
Under normal circumstances, an ombudsperson would go to the facility and talk to patients and could do so without announcing the visit in advance. Since visits are restricted for infection control reasons, they have to work through staff to speak to residents or to ask questions, which isn’t optimal. And they aren’t able to make direct observations.
“It makes our job much more challenging,” Cyrill said.
At the North Salem facility, which has had about a dozen new residents admitted or transfered from other facilities, the staff has given “virtual tours” over the phone to family members or prospective residents who were in the hospital, Stratmann said. The company also invested in technology that won’t replace face-to-face visits but enables more family contact and the ability and for staff to help keep residents’ spirits up by making videos of activities, like dancing and singing, to keep them connected with the local community.
In addition, Stratmann said they walk families through the infection control procedures and share techniques they have implemented to improve health outcomes for patients with COVID-19 including, when appropriate:
Treating residents with anticoagulant medications to reduce the risk of blood clots and strokes, which has been a factor in some COVID-19-related fatalities.
Practicing “proning” or positioning residents, while awake, flat on their belly and chest to reduce the buildup of fluid in lung tissue and reduce the risk of Acute Respiratory Distress Syndrome, which has been associated with many COVID-19 fatalities.
The idea of putting their beloved grandfather in a nursing home was gut-wrenching
Choosing home
For Bondar’s family, the idea of putting their beloved grandfather in a nursing home was gut-wrenching, especially as visitation was curtailed to limit the virus’ spread. He speaks Russian, his native language, and would not have been able to communicate well with the staff caring for him.
“It felt like admitting him [to a facility] would be like saying goodbye,” Bondar said. “Like leaving him to die.”
Bondar’s family ultimately decided to care for her grandfather at home, in his Mayfield Heights senior highrise, where they could limit his exposure to the virus.
Before his fall, an aide visited for about eight hours a week. After the Ohio’s “stay at home” order was put in place March 23, Bondar and her mother were able to work from home and pitch in with care.
The advice of the Clinic’s Steven Schwartz led them to a hospice program, which helped the family find additional aides, including one who speaks Russian, as well as a hospital bed for safer sleeping and a wheelchair.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
The home care route isn’t the easiest but Bondar said the family feels like they have more contact and control over the quality of care.
“We’ll do this as long as we can manage it,” Bondar said.
Anecdotally, it is a choice more families are making: the decision to use home care or even pull family members out of nursing homes out of fear or because they miss them and can’t visit, Steven Schwartz said.
“Sometimes it’s appropriate. But sometimes, even given everything, it may be safer to have your family member there to get stronger and get the necessary care,” said Steven Schwartz. “I would really try to balance the benefit of going to a nursing home versus the risk.”
Patients with dementia or Alzehimer’s may be unsafe going back home.
Patients with dementia or Alzehimer’s may be unsafe going back home, he said, and families may need to decide if a nursing home really is the safer place.
One of the first orders Ohio put in place to prevent the spread of COVID-19 was to halt in-person visitation in more than 900 nursing and long-term care facilities. The state is not yet ready to lift those restrictions and resume visits in those settings, Gov. Mike DeWine said, but on June 8 will start allowing outdoor visits at assisted living facilities care centers for individuals with disabilities.
“We are not to nursing homes yet and I know that causes anguish for a lot of people who are watching this but we’re trying to do this so that we don’t increase the COVID inside the nursing homes or the assisted living or the immediate care facilities,” DeWine said during a May 28 briefing.
Decisions made harder
Figuring out what kind of care might be best for a patient has become more challenging, too.
Previously, nurses and social workers would visit clients in their homes to assess how they functioned – whether they could independently bathe, cook and grocery shop, said Theresa Foster, a nurse and licensed social worker at Western Reserve Area Office on Aging.
They relied on conversations with clients and family and also observations of the environment in the home and possible risks, said Foster, who runs the agency’s resource center.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Now, those assessments are done by phone and can be done successfully, but it is more difficult, Foster said.
At UH’s hospitals, medical staff use a scoring system to determine the best place for a patient being discharged, said Dr. Sean Cannone, UH’s medical director for population health.
Patients are assessed on their ability to perform daily tasks and on their cognitive abilities.
“We’re trying as much as we can to get patients home if at all possible,” he said. The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
The goal is to provide patients with resources so they can receive care in whichever setting they prefer.
“We want to respond to what people really want for their own care,” Cannone said.
The shift started before COVID-19 cases surfaced but has accelerated as more families worry about potential exposure to the virus in congregate living situations.
As technology has advanced, the capabilities of what can be done in a patient’s home has also increased. In March, UH introduced a new patient management system, Massimo SafetyNet, for remote monitoring.
When patients are released from the emergency room or from a COVID-19 floor, providers now put a bluetooth sensor on their wrist — it looks like an Apple Watch — that streams data about a patient’s vitals to a central monitoring center, said Jonathan Sague, UH’s vice president of clinical operations. That way, providers can make sure a patient is safe at home.
Douglas Beach is the chief executive officer at Western Reserve Area Office on Aging
Douglas Beach, chief executive officer at Western Reserve Area Office on Aging, has had firsthand experience weighing care decisions amid COVID-19 worries. His mother is rehabilitating in a nursing home after a six-week hospital stay related to a heart condition.
Not being able to visit her in the hospital or the facility has been hard, Beach said. He and his brother, who is a doctor, had to make all of the arrangements by phone, including figuring the best way to transport her that would have the lowest risk of exposure to the virus.
“Home and community-based services is what I do,” Beach said. Part of his mission is to advocate for the setting that allows for any person, whether they are older adults or live with a disability, to be as independent as possible .
But for his mother, a nursing facility was the right choice because she needed 24-hour care that her family could not provide at home.
Beach said nursing homes have had to deal with an unprecedented set of circumstances: a new virus, initial unknowns about transmission and populations at extremely high risk for complications.
Nursing homes will continue to play a vital role and will remain the best option for people who need more care than can be safely provided at home, Beach said.
For the more than 9,500 clients his agency serves in Cuyahoga, Geauga, Lake, Lorain and Medina counties, delivering care at home, with health aides, nurses and community and family supports, has proven a low risk. As of mid-May only 35 clients had tested positive for the virus, he said. That is roughly 0.3% of clients, though not all clients are tested.
Managing COVID-19
Cuyahoga County nursing homes have been paired with one of the area’s three largest hospital systems during the pandemic, Campbell said. The hospitals help the facilities both prepare for and respond to COVID-19 cases.
“The goal is when you have one patient in a nursing home with COVID is to make sure you don’t end up with 30 patients with COVID,” Campbell said.
UH developed what is being called a playbook for local nursing homes. The playbook gives facilities a plan for how to respond if there’s a COVID-19 outbreak on-site, said Sague, who works as a firefighter and medic on the weekends.
“It can be pretty startling and pretty alarming if they’re not ready for it,” Sague said.
The playbook gives guidelines on screening, triaging, determining exposure, testing and isolating those who test positive, as well as how to get personal protective equipment, increase staffing and to eventually reopen safely, Sague said.
Once a case is identified at a facility, what is known as an intercept team is dispatched — either virtually or in person — to help a nursing home handle it, he said.
Patrick Schwartz, director of strategic communications for LeadingAge Ohio, a long-term care trade association, said access to testing and safety equipment has been a consistent problem for Ohio’s nursing homes.
But in the past month or so, the state has made “a definite shift” and started prioritizing testing at nursing homes, which is helping, he said.
Patrick Schwartz said he hoped the expanded testing would enable facilities to test their entire population— of residents and staff — so they can better limit the spread of the virus.
Throughout Ohio, populations that have received mass testing — health care workers, first responders, those incarcerated and those in nursing homes — have had higher numbers of positive cases. Many people with COVID-19 are asymptomatic, so it is unknown if they have the virus until they are tested.
“Since this pandemic first reared its head, it was clear to long-term care providers that the front lines would be in long-term care,” Patrick Schwartz said. The populations at those congregate living facilities, many of whom are older and have multiple medical conditions, are among the most vulnerable for complications from COVID-19, he said.
In Cuyahoga County, and elsewhere, local health departments have deployed limited testing resources to nursing homes quickly in hopes of limiting spread in and between facilities and given guidance to homes about how to isolate patients and trace exposures between facilities to limit the spread of infection.
Cuyahoga County Health Commissioner Terry Allan said nursing homes try to guard against outbreaks but have varying degrees of resources. The assistance from the National Guard will allow more residents and staff at facilities in Northeast Ohio to be tested, he said.
Support for this project was provided by the Center for Community Solutions.
Questions to ask:
How can family members stay in touch with residents while visiting is restricted?
Does staff facilitate video visits? Is window visiting allowed?
How often will the facility provide updates on a resident’s condition?
How much COVID-19 testing is being done? Is the facility proactively testing patients or only those with symptoms?
Are private rooms available?
Do staffing ratios allow for residents to be taken outside?
Are residents currently restricted to rooms?
Are separate units and staffs used for COVID-19-positive patients and COVID-19-negative patients?
How does the facility work to limit COVID-19 complications?
The weekly press release from Ohio Governor Mike DeWine
For the week ending April 24, 2020
Throughout the week, Ohio Governor Mike DeWine was joined by Lt. Governor Jon Husted and Ohio Department of Health Director Amy Acton M.D., MPH, to announce decisions made regarding the spread of Coronavirus (COVID-19) throughout Ohio.
On Monday, Governor DeWine announced that K-12 schools in Ohio will remain closed for the rest of the 2019-2020 academic year. At this time, no decisions have been made regarding whether or not schools will reopen in the fall. *
Governor DeWine announced a new Minority Health Strike Force because COVID-19 is disproportionately impacting minority groups in Ohio and across the country. A list of individuals serving on the Minority Health Strike Force can be found here.
Governor DeWine directed the Ohio Department of Health to collect more specific information regarding cases of COVID-19 in Ohio nursing homes, assisted living facilities, and hospitals. This is in addition to comprehensive data already published on coronavirus.ohio.gov.
Governor DeWine also directed the Department of Health to modify the Ohio Disease Reporting System to accurately collect case information for direct care providers at hospitals who have tested positive for COVID-19. The data, which will be available soon on coronavirus.ohio.gov, will be listed by each hospital.
Governor DeWine announced that LabCorp and Quest currently have no backlog of testing samples and have added more testing capacity. In response to the private laboratories’ improved turnaround times, the Ohio Department of Health will again allow hospitals to utilize commercial laboratories in addition to hospital laboratories performing COVID-19 testing.
On Tuesday, Governor DeWine announced that a new testing reagent, which is a compound used to determine if COVID-19 is present in a sample, has been approved by the U.S. Food and Drug Administration (FDA).
A new strike force team, led by former Ohio governors Richard Celeste and Bob Taft, will work to find more reliable sources of reagent and testing supplies for COVID-19 testing in Ohio. The new Testing Strike Team will also include leaders from business, academia, and public health to help Ohio source these testing reagents and supplies.
The Ohio Department of Agriculture has waived the required $50,000 local match for the Agricultural Society Facilities Grant Program. Fair managers have until May 30th to apply via the Ohio Department of Agriculture’s website.
JobsOhio, Peoples Bank (headquartered in Marietta) and the recently-merged First Federal Bank and Home Savings Bank (headquartered in Defiance and Youngstown) announced a new partnership to support those banks’ existing small business clients in Ohio.
The partnership will help small businesses maintain operations and payroll during the COVID-19 pandemic. JobsOhio has committed up to $50 million to assist Peoples Bank and First Federal-Home Savings Bank.
Additionally, a total of more than 170,000 checks will be mailed to Ohio employers over the next five days. Less than two weeks ago, the Ohio Bureau of Workers’ Compensation board of directors approved to send up to $1.6 billion in dividends to Ohio employers. This dividend is intended to ease the impact of COVID-19 on Ohio’s business community and the economy.
On Wednesday, Dr. Acton announced an order that directs healthcare providers in hospitals and outpatient surgery centers to reassess procedures and surgeries that were postponed.
On March 17, Dr. Acton issued an order postponing elective surgeries to conserve critical personal protective equipment (PPE) and to open bed space needed to care for COVID-19 patients. The new order directs healthcare professionals to review any postponed procedures or surgeries with their patients.
The Ohio Department of Mental Health and Addiction Services (MHAS) announced the launch of a new mental health COVID CareLine for Ohioans.
Trained staff will be available to provide emotional assistance to anyone struggling with mental health concerns due to the ongoing stress of the pandemic.
The number to call is 1-800-720-9616. All calls will be confidential.
On Thursday, Governor DeWine and Lt. Governor Husted invited Mark Weir, Ph.D., an assistant professor of Environmental Health at The Ohio State University, to discuss how health risks change as changes are made to the environment.
Dr. Weir explained that cough or sneeze droplets containing the virus spread through contact with others or contact with contaminated surfaces. He explained that minimizing the spread of the disease as Ohio begins the long process of reopening depends on personal and environmental controls. Personal precautions include interrupting the infection process by practicing good hand hygiene and wearing masks.
Employers must take precautions by disinfecting surfaces often and maintaining distance between individuals. Finally, facility and building management can help interrupt the infection process by managing airflow and air filters.
“Since COVID-19 can live up to 72 hours on plastics and stainless steel, it will take a combination of efforts from all of us to interrupt the disease process,” said Dr. Weir.
On Friday, Governor DeWine announced that members of the newly formed Testing Strike Team, led by former Governors Celeste and Taft, have reached an agreement with Thermo Fisher, a company that makes reagent, that will substantially expand COVID-19 testing capacity in Ohio.
As a result of collaborative efforts through the Ohio Manufacturing Alliance to Fight COVID-19, Governor DeWine announced that ROE Dental Laboratory in Cleveland will manufacture up to 1 million testing swabs to support Ohio’s testing efforts.
This testing will dramatically increase Ohio’s ability to test in our priority areas, including nursing homes, hot spots, congregate living settings, food and grocery stores, and essential manufacturing facilities.
As part of Ohio’s offense strategy, Governor DeWine announced that Ohio has started working with Massachusetts-based Partners in Health. Partners in Health will bring needed resources to Ohio to help increase the ability to trace contact exposure to the virus.
Additionally, Governor DeWine announced that the state will cover the costs to keep more than 200 youth who are aging out of foster care in the foster care system until the COVID-19 pandemic ends.
As of Friday afternoon, there were 15,169 confirmed and probable cases of COVID-19 in Ohio and 690 confirmed and probable COVID-19 deaths. A total of 3,053 people have been hospitalized, including 920 admissions to intensive care units. In-depth data can be accessed by visiting coronavirus.ohio.gov.
For more information on Ohio’s response to COVID-19, visit coronavirus.ohio.gov or call 1-833-4-ASK-ODH.
EDITOR’S NOTE: Loveland school buildings are closed to the public, however remote learning is being conducted at the Loveland City School District.
The “Ohio Attorney General’s Sexual Assault Kit Tracking System” will give those who have undergone a sexual assault forensic examination the option to track the status of their rape kit evidence online.
Columbus, Ohio – Attorney General Mike DeWine announced Thursday that his office is developing a statewide system that will increase transparency surrounding the collection, submission, and analysis of sexual assault kit evidence in Ohio.
The “Ohio Attorney General’s Sexual Assault Kit Tracking System” will give those who have undergone a sexual assault forensic examination the option to track the status of their rape kit evidence online.
“Sexual assault survivors have already gone through unimaginable trauma, and not knowing where their cases stand can be agonizing,” said DeWine. “This new system will empower survivors by giving them the ability to instantly and anonymously find out where their evidence is located and whether or not it has been submitted for testing.”
By entering a barcode number into the free, online program, survivors who choose to use the system will be able to follow their evidence as it proceeds from collection at a medical facility, to inventory at a law enforcement agency, to analysis at a crime lab, and to storage or destruction.
By entering a barcode number into the free, online program, survivors who choose to use the system will be able to follow their evidence as it proceeds from collection at a medical facility, to inventory at a law enforcement agency, to analysis at a crime lab, and to storage or destruction.
New legislation introduced by State Senator Stephanie Kunze (R-Hilliard) and State Representative Dorothy Pelanda (R-Marysville) seeks to require all agencies involved in the chain-of-custody of sexual assault kits to participate in the tracking program.
“As we continue to help and encourage victims of sexual assault to rebuild their lives, it is imperative that we provide them the ability to check the status of the testing of their rape kits quietly and discreetly,” said Senator Kunze. “Affording them the opportunity to do so in a safe, secure manner ensures their privacy. We can allow survivors to continue moving forward with the option to check on the progress to help with the emotional healing and journey to moving forward from their horrific experience.”
“Attorney General DeWine and his office have demonstrated tremendous leadership and diligence when it comes to this issue. The bills introduced this week in the House and Senate represent a crucial next step in the process,” said Representative Pelanda. “I look forward to working with Attorney General DeWine, my great colleague Senator Kunze, and my brothers and sisters in the House of Representatives as we move forward with this legislation.”
The advisory group will include victim advocates, sexual assault nurse examiners, law enforcement, prosecutors, and representatives from hospital associations and crime laboratories.
DeWine is also creating an advisory group to study best practices and provide advice on how Ohio’s tracking system should operate. The advisory group will include victim advocates, sexual assault nurse examiners, law enforcement, prosecutors, and representatives from hospital associations and crime laboratories. The members of the advisory group, who will be announced at a later date, will give special consideration to protecting the privacy of survivors who use the system.
“We are excited to see this initiative coming from the Ohio Attorney General’s Office,” said Rosa Beltre, executive director of the Ohio Alliance to End Sexual Violence. “It is important to reform how rape kits are handled and tracked in the state of Ohio, despite the many challenges and difference of opinion. We collectively can choose to do nothing because of funding and road blocks, or as we have done today, we can choose to take steps within our circle of influence to make a difference. We owe this to every survivor in our state.”
The development of the program, as well as any maintenance and equipment, will be financed through Victim of Crime Act (VOCA) funding. VOCA funds, which are administered by the Ohio Attorney General’s Office, are from federal settlements, fines, and fees and must be used to enhance victim rights and services.
“This new tracking system will also help ensure that an accumulation of untested rape kits never happens in Ohio again,” said Attorney General DeWine. “Survivors expect their kits to be submitted for analysis in a timely manner, and this new program will increase accountability and transparency throughout the entire process.”
To date, Attorney General DeWine’s SAK Testing Initiative has led to 5,071 hits in the Combined DNA Index System (CODIS), and hundreds of attackers have been prosecuted according to DeWine’s office. In response to the success of the initiative, new law was enacted in 2015 requiring that law enforcement agencies in Ohio submit sexual assault kit evidence to a crime laboratory within 30 days.






 Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.
Those assessments were used to determine whether a person could safely remain at home with community support or whether they needed facility-level care and what resources, whether subsidized or private, existed to pay for the services.