Loveland Magazine received this Guest Column from the parent of a Loveland school student who asked us not to reveal their identity and to go one further step, besides sharing the sentiment of her writing – to help protect all of the “health compromised children” that need to attend school next week.
Most of you don’t know what it’s like to have a medically fragile child. Most of you never will.
Most of you don’t know what it’s like to beg God to let your child live another day... thankfully, most of you never will.
Most of you do not know what the scene of life-saving measures on your child looks like - and thank God, most of you never will.
But unfortunately, for some of us parents - we do know all of these moments and they never leave us. They are forever ingrained in our memory - you can see, smell, hear and taste these moments.
Always.
Forever.
I’ve come to realize that most of you don’t realize what you're asking of parents like me - with young, medically fragile children.
You can’t possibly realize what you’re asking... because I cannot wrap my head around it - if you do realize what you're asking of me - how can I possibly wrap my head around the fact that I’ve been surrounding myself with so many people that would dare have such an ask.
So many fake promises like “I’m here! It takes a village”.
I sit back and think-shame on you. HOW DARE YOU. But then I remind myself, there is no way they realize their “ask”. I won’t call you selfish - because there is no way you really understand what you’re asking - and if you do, then it’s a step beyond selfish- it’s evil... and may God help you.
We are asking one simple thing, parents like me — but you, you’re asking for my world.
We ask just one simple thing - but you, you are asking for us to choose risk.
We are asking for one thing - a very simple thing, indeed.
But you... you are asking something far too big- something far outside of our reach.
We are asking you for one simple thing... a mask. Please, we ask - it’s just a mask...
But you, oh YOU... you cannot possibly realize it, can you?! You think you’re asking for choice... you think you have this right... but what you don’t realize, you can’t possibly realize — is that you’re asking me to risk my child’s life. You’re asking me to not put up a fight.
You’re asking me to risk the very depth of my being - my reason for living - you are asking me to sacrifice all that we’ve done - and asking us to risk our children’s health... and all we ask of you is one SIMPLE thing... please mask up, to help protect the children. Send your child to school with a mask... you may save a life.
If you’re reading this and getting angry, still not getting our message, then it may be time to take a long look in the mirror and start asking yourself some hard questions.
Please stop demanding we risk our children’s life.
Our ask is simple.
And your ask, well it’s inconceivable.
The letter below was sent to the Principal of St. Columban School today. A similar letter was sent to Superintendent Broadwater and the Loveland School Board yesterday.
Matt and Stefanie Laufersweiler have students enrolled in both school systems.
Dear Mrs. Muchmore,
I’m writing to urge you as you review plans for safely opening St. Columban School this year to not let the wants of parents steer you away from the objective guidance of healthcare professionals when putting measures in place to protect the health of our children. There are many who have expressed vocally their desire to return to school “unmasked” out of a desire to return to life as it was pre-COVID. However desirable this may seem, it does not consider the fact that case numbers are increasing and all counties in the area are now considered to be at the highest category for level of spread (https://www.cincinnati.com/…/covid-19-ohio…/5505300001/ ). In addition, with the Delta variant in particular, an increasing number of those infected are children (https://www.usatoday.com/…/covid-vaccines…/5532551001/ ) which has resulted in schools in other states having to move to remote learning very early in the school year due to COVID-19 outbreaks.
Last year St. Columban did an excellent job ensuring that spread in school was minimal by enforcing masking and distancing policies following the guidelines of healthcare professionals before vaccines were available. As you consider and pray over the best way to open school this year, we ask that you keep in mind the current spread and the recommendations of healthcare professionals.
To this point, the Ohio Department of Health released revised recommendations for schools K-12 on July 27th, and in doing so reference the current statistics and the effectiveness of measures used last school year to keep the children safe while ensuring they continue to get a quality education.
Encouragement of vaccination for those eligible is also important; however, many children that will be in the school are not eligible for vaccination at this time. The key factor to help protect those children is universal masking while indoors, until those kids have the opportunity to be vaccinated and the spread of COVID-19 is back under control.
It is also important to note that masking as a “personal choice” is ineffective in that the reason masks are effective is that they help to contain the spread from those who are unknowingly infected, preventing the aerosolization of the virus – they do little to help protect the individual wearer from already aerosolized virus (An evidence review of face masks against COVID-19 https://www.pnas.org/content/118/4/e2014564118 “Because many respiratory particles become smaller due to evaporation, we recommend increasing focus on a previously overlooked aspect of mask usage: mask wearing by infectious people (“source control”) with benefits at the population level, rather than only mask wearing by susceptible people, such as health care workers, with focus on individual outcomes.”).
This is not simply a desire of a parent; it is the objective recommendation of healthcare professionals to protect the health of our children and ensure that they can remain in school and involved in the extracurricular activities that they love. It is the responsibility of the school and the community to help keep our kids safe, even if it means the measures required to do so are not always popular.
Loveland, Ohio – The tracking system of the Centers for Disease Control and Prevention (CDC) has now moved Hamilton County, Ohio to the highest level of warning for the transmission of COVID 19.
Clermont and Warren Counties remain in the “High” rate of transmission range.
How do levels of community transmission affect schools?
UPDATE: Given new evidence on the B.1.617.2 (Delta) variant, CDC has updated the guidance for fully vaccinated people. CDC recommends universal indoor masking for all teachers, staff, students, and visitors to K-12 schools, regardless of vaccination status. Children should return to full-time in-person learning in the fall with layered prevention strategies in place.CDC Guidance for COVID-19 Prevention in K-12 Schools
Updated Aug. 5, 2021
Key Takeaways
Students benefit from in-person learning, and safely returning to in-person instruction in the fall 2021 is a priority.
Vaccination is the leading public health prevention strategy to end the COVID-19 pandemic. Promoting vaccination can help schools safely return to in-person learning as well as extracurricular activities and sports.
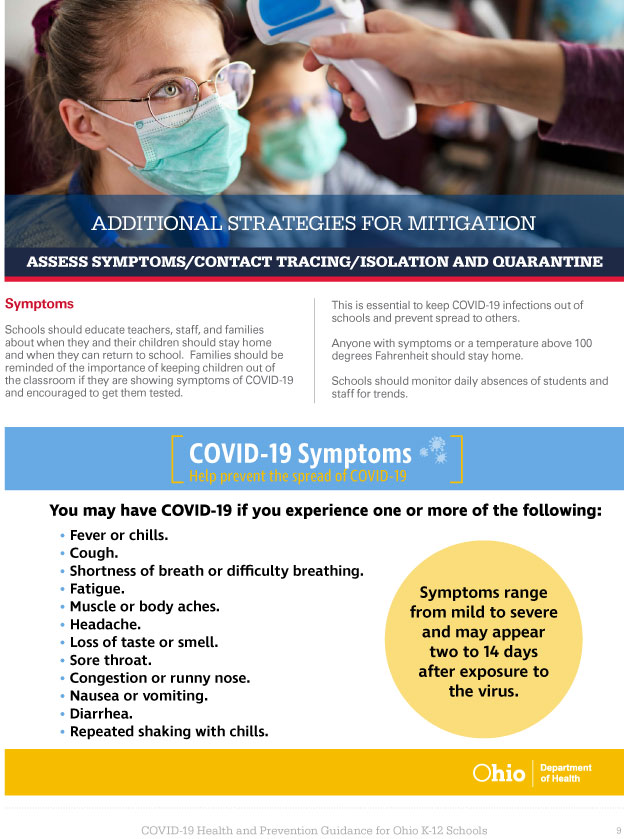
Due to the circulating and highly contagious Delta variant, CDC recommends universal indoor masking by all students (age 2 and older), staff, teachers, and visitors to K-12 schools, regardless of vaccination status.
In addition to universal indoor masking, CDC recommends schools maintain at least 3 feet of physical distance between students within classrooms to reduce transmission risk. When it is not possible to maintain a physical distance of at least 3 feet, such as when schools cannot fully re-open while maintaining these distances, it is especially important to layer multiple other prevention strategies, such as screening testing.
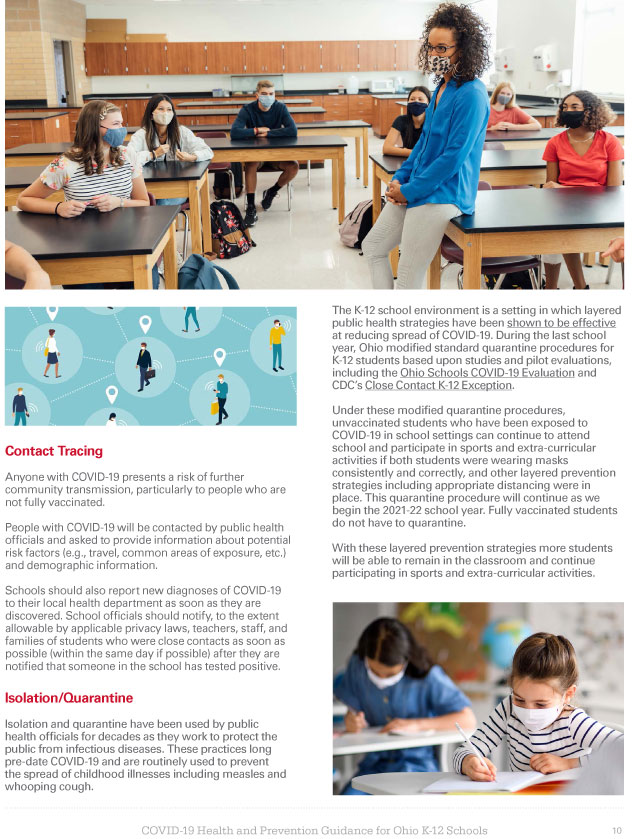
Screening testing, ventilation, handwashing and respiratory etiquette, staying home when sick and getting tested, contact tracing in combination with quarantine and isolation, and cleaning and disinfection are also important layers of prevention to keep schools safe.
Students, teachers, and staff should stay home when they have signs of any infectious illness and be referred to their healthcare provider for testing and care.
Many schools serve children under the age of 12 who are not eligible for vaccination at this time. Therefore, this guidance emphasizes implementing layered prevention strategies (e.g., using multiple prevention strategies together consistently) to protect students, teachers, staff, visitors, and other members of their households and support in-person learning.
Localities should monitor community transmission, vaccination coverage, screening testing, and occurrence of outbreaks to guide decisions on the level of layered prevention strategies (e.g., physical distancing, screening testing).
Summary of Recent Changes
Updates as of August 4, 2021
Updated to recommend universal indoor masking for all students, staff, teachers, and visitors to K-12 schools, regardless of vaccination status.
Added recommendation for fully vaccinated people who have a known exposure to someone with suspected or confirmed COVID-19 to be tested 3-5 days after exposure, regardless of whether they have symptoms.
Loveland, Ohio – The Loveland City School District Board of Education met tonight. Without a motion coming forward to change or alter the “Use of Face Coverings/Masks” policy, the Board let stand the current policy of the District.
Below is the current policy.
Revised June 3, 2021
8450.01 – USE OF FACE COVERINGS/MASKS
The Loveland Board of Education is committed to providing students, staff, and visitors with a safe and healthy environment.
On May 12, 2021, Ohio Governor Mike DeWine lifted the State’s COVID – 19 mask requirements, including the requirement of face coverings inside public buildings, effective June 2, 2021 Furthermore, he declared that local school districts will make their own determinations on Covid-19 mitigation efforts, including the wearing of masks and/or face shields.
As of the adoption date, June 3, 2021, of this updated policy, unless required by additional mandates, the decision to wear face coverings/masks on school buses, in school buildings, or at other school events, will be left to adult individuals and parents/guardians of K-12 students. The Loveland City Schools will continue to follow COVID-19 mitigation protocols to maintain a healthy environment for students, staff, and visitors and will continue to provide recommendations for personal protection from the spread of infectious diseases.¶
In order to maintain a healthy environment, the Board will follow any mandates set forth by the Ohio Governor, Ohio State Health Department, Hamilton County Health Department, and Ohio Department of Education, (“Directing Entities”) as it relates to protecting the health of students, staff and visitors. When any of these Directing Entities requires staff, students, and visitors to wear face coverings/masks while attending school, reporting to work at a school, or visiting a school, the District’s Administration will follow and enforce such directives.
David Miller is the Publisher and Editor of Loveland Magazine
By David Miller
Dear Loveland School Board.
Given that COVID infections caused by the now predominant delta variant are likely to go undetected and children attending school with what appears to be a mild cold, what measures, if any, do you propose to use to prevent the spread of COVID-19 throughout the Tiger school community?
The predominant delta variant is much more contagious than the version of COVID-19 Loveland school children faced last year.
Here is a list of things to consider and do before your meeting on Tuesday, August 10 – eight days before classes begin for the school year. I have provided the resource materials below that you will need to complete your assignment.
You know this but does it bear repeating? Loveland students eleven years old and younger cannot currently receive any benefit a vaccination will provide.
Only approximately 18% of our students who are eligible for a vaccine are fully vaccinated.
The tracking system of the Centers for Disease Control and Prevention (CDC) has now moved Clermont and Warren Counties to the highest level of warning for the transmission of COVID 19. Hamilton County remains in the “Substantial” range.
There will be no remote learning opportunities (Remote Academy) for Loveland teachers or students as all school buildings will return to full capacity in-person classes in August. Find out how many more students will be attending each building and riding buses as classes begin.
Find out how many students, staff, and teachers became infected and how many were quarantined last school year when there were far fewer persons in the buildings and on buses than there will be this year.
Review the comprehensive study ($66K “Pandemic Preparedness and Planning” services) that you purchased before school began last year. Review which of the recommended COVID protocols were implemented and whether or not you are going to abandon them as school starts on August 18.
Your current policy states that you will follow any “mandates” of a list of what you call your “Directing Entities”. Since none of these “Directing Entities” have mandated protocols and nothing in current Ohio law prevents you from adopting any recommendation you choose – review their recommendations and choose one.
Below is a list of what your “Directing Entities” are currently recommending for K-12 schools.
Also, below for your review, are the recommendations contained in the $66,000 report you purchased.
With all due respect, none of you or your staff are smarter or have any greater insight as to what is the best way to start this school year than the medical and scientific community of your Directing Entities.
And, with all due respect to the parents of the District, “parental choice” of your child wearing a mask or not – is not your decision to make. You can be the loudest voice in the classroom of social media, but just as the elected Board of this District relies on known experts to decide which textbooks teachers use or what is served in the cafeteria – providing a healthy classroom is in their job description.
Board, please follow the latest advice from the health experts, your “Directing Entities” and from your own “consultant experts” that you hired in 2020.
Let’s get back to school. Let’s do so in a way that fully protects our children, teachers, and our friends that work as District staff. Don’t allow any of them to be put in the potentially lethal classroom petri dish experiment of this new delta variant.
“It is strongly recommended that schools implement masking.”
Loveland, Ohio – When asked, this morning to provide Loveland Magazine with the current Board of Health guidance for covid 19 protocol for K-12 schools “Mike Samet, the Public Information Officer for Hamilton County Public Health responded, “We are following the Ohio Dept. of Health guidelines (attached) until we develop our own, if necessary.”
The current Loveland school protocol reads in part, “…the Board will follow any mandates set forth by the Ohio Governor, Ohio State Health Department, Hamilton County Health Department, and Ohio Department of Education, (“Directing Entities”) as it relates to protecting the health of students, staff and visitors.”
There will be no remote learning opportunities (Remote Academy) for Loveland teachers or students as all school buildings will return to full capacity in-person classes in August.
Samet referred Loveland Magazine to the Ohio Dept. of Health (ODH) guidelines which are currently Hamilton County Health Department’s as well.
The ODH guidelines begin with this opening introduction:
As schools get ready for the 2021-22 academic year, the ongoing health and safety of students, staff, and volunteers remains paramount. While great strides have been made in controlling the spread of COVID-19, the virus remains a health threat.
Although children are less likely to get severely ill from COVID-19 compared with adults, they are at risk of being infected with the virus that causes COVID-19, getting sick from COVID-19, spreading the virus to others, and having severe health outcomes.
Because children 11 and younger cannot be vaccinated and less than a third of children 12 to 17 are fully vaccinated, it is strongly recommended that schools implement masking for students layered with other prevention strategies to protect people who are not fully vaccinated.
The Delta variant is rapidly becoming dominant in Ohio. It is highly transmissible, increasing risk, especially for those who are unvaccinated. Because the Delta variant spreads so quickly, these strategies to reduce transmission in school are critically important to protect students, teachers, staff, and communities.
As students head back to school, the Ohio Department of Health (ODH) recommends following the same layered prevention strategies that were remarkably effective at controlling COVID-19 last school year:
Strongly recommend vaccinations for staff and eligible students. Vaccines are our best tool to protect students and prevent the spread of the virus.
Wearing masks. Masks have been proven to be extremely effective in slowing the spread of the virus. Ohio researchers conducted an evaluation last year that showed that masking helped control the spread of the virus in Ohio schools. ODH strongly recommends that those who are unvaccinated wear masks while in school.
Additional measures including improving ventilation, maximizing distance between people, and practicing good hygiene, among others.
Consistent implementation of these core prevention measures helped limit the spread of COVID-19 in the classroom during the 2020-21 academic year. Continuing to follow these recommendations will protect students as much as possible.
As the next school year begins, there needs to be a continued focus on keeping students safe, since not all students will have the opportunity or be eligible to be vaccinated before the start of the next school year. – American Academy of Pediatrics
The AAP strongly advocates that all policy considerations for school plans should start with the goal of keeping students safe and physically present in school.
Purpose and Key Principles
The purpose of this guidance is to continue to support communities, local leadership in education and public health, and pediatricians collaborating with schools in creating policies for safe schools during the COVID-19 pandemic that foster the overall health of children, adolescents, educators, staff, and communities and are based on available evidence. As the next school year begins, there needs to be a continued focus on keeping students safe, since not all students will have the opportunity or be eligible to be vaccinated before the start of the next school year. Since the beginning of this pandemic, new information has emerged to guide safe in-person learning. Remote learning highlighted inequities in education, was detrimental to the educational attainment of students of all ages, and exacerbated the mental health crisis among children and adolescents. 1,2 Opening schools generally does not significantly increase community transmission, particularly when guidance outlined by the World Health Organization (WHO),3 United Nations Children’s Fund (UNICEF), and Centers for Disease Control and Prevention (CDC) is followed. 4,5 There are still possibilities for transmission of SARS-CoV-2, especially for individuals and families who have chosen not to be vaccinated or are not eligible to be vaccinated. In addition, SARS-CoV-2 variants have emerged that may increase the risk of transmission and result in worsening illness. However, the AAP believes that, at this point in the pandemic, given what we know about low rates of in-school transmission when proper prevention measures are used, together with the availability of effective vaccines for those age 12 years and up, that the benefits of in-person school outweigh the risks in almost all circumstances. Along with our colleagues in the field of education,6the American Academy of Pediatrics (AAP) strongly advocates for additional federal assistance to all schools throughout the United States, irrespective of whether the current local context allows for in-person instruction.
Schools and school-supported programs are fundamental to child and adolescent development and well-being and provide our children and adolescents with academic instruction; social and emotional skills, safety, reliable nutrition, physical/occupational/speech therapy, mental health services, health services, and opportunities for physical activity, among other benefits.7 Beyond supporting the educational development of children and adolescents, schools can play a critical role in addressing racial and social inequity. As such, it is critical to reflect on the differential impact the COVID-19 pandemic and the associated school closures have had on different racial and ethnic groups and populations facing inequities. Disparities in school funding, quality of school facilities, educational staffing, and resources for enriching curricula among schools have been exacerbated by the pandemic. Families rely on schools to provide a safe, stimulating, and enriching space for children to learn; appropriate supervision of children; opportunities for socialization; and access to school-based mental, physical, and nutritional health services.
Everything possible must be done to keep students in schools in-person. Many families did not have adequate support to the aforementioned educational services, and disparities, especially in education, did worsen, especially for children who are English language learners, children with disabilities, children living in poverty, and children who are Black, Hispanic/Latino, and American Indian/Alaska Native. 8,9,10,11
The AAP strongly recommends that school districts promote racial/ethnic and social justice by promoting the well-being of all children in any school COVID-19 plan, with a specific focus on ensuring equitable access to educational supports for children living in under-resourced communities.
It is critical to use science and data to guide decisions about the pandemic and school COVID-19 plans. All school COVID-19 policies should consider the following key principles and remember that COVID-19 policies are intended to mitigate, not eliminate, risk. Because school transmission reflects (but does not drive) community transmission, it is vitally important that communities take all necessary measures to limit the community spread of SARS-CoV-2 to ensure schools can remain open and safe for all students. The implementation of several coordinated interventions can greatly reduce risk:
All eligible individuals should receive the COVID-19 vaccine.
It may become necessary for schools to collect COVID-19 vaccine information of staff and students and for schools to require COVID-19 vaccination for in-person learning.
Adequate and timely COVID-19 vaccination resources for the whole school community must be available and accessible.
All students older than 2 years and all school staff should wear face masks at school (unless medical or developmental conditions prohibit use).
The AAP recommends universal masking in school at this time for the following reasons:
a significant portion of the student population is not eligible for vaccination
protection of unvaccinated students from COVID-19 and to reduce transmission ▪ lack of a system to monitor vaccine status among students, teachers and staff
potential difficulty in monitoring or enforcing mask policies for those who are not vaccinated; in the absence of schools being able to conduct this monitoring, universal masking is the best and most effective strategy to create consisent messages, expectations, enforcement, and compliance without the added burden of needing to monitor vaccination status
possibility of low vaccination uptake within the surrounding school community
continued concerns for variants that are more easily spread among children, adolescents, and adults
An added benefit of universal masking is protection of students and staff against other respiratory illnesses that would take time away from school.
Adequate and timely COVID-19 testing resources must be available and accessible.
It is critically important to develop strategies that can be revised and adapted depending on the level of viral transmission and test positivity rate throughout the community and schools, recognizing the differences between school districts, including urban, suburban, and rural districts.
School policies should be adjusted to align with new information about the pandemic; administrators should refine approaches when specific policies are not working.12
Schools must continue to take a multi-pronged, layered approach to protect students, teachers, and staff (ie, vaccination, universal mask use, ventilation, testing, quarantining, and cleaning and disinfecting). Combining these layers of protection will make in-person learning safe and possible. Schools should monitor the implementation and effectiveness of these policies.
Schools should monitor the attendance of all students daily inclusive of in-person and virtual settings. Schools should use multi-tiered strategies to proactively support attendance for all students, as well as differentiated strategies to identify and support those at higher risk for absenteeism.
School districts must be in close communication and coordinate with state and/or local public health authorities, school nurses, local pediatric practitioners, and other medical experts.
School COVID-19 policies should be practical, feasible, and appropriate for child and adolescent’s developmental stage and address teacher and staff safety.
Special considerations and accommodations to account for the diversity of youth should be made, especially for populations facing inequities, including those who are medically fragile or complex, have developmental challenges, or have disabilities. Children and adolescents who need customized considerations should not be automatically excluded from school unless required in order to adhere to local public health mandates or because their unique medical needs would put them at increased risk for contracting COVID-19 during current conditions in their community.
School policies should be guided by supporting the overall health and well-being of all children, adolescents, their families, and their communities and should also look to create safe working environments for educators and school staff. This focus on overall health and well-being includes addressing the behavioral/mental health needs of students and staff.
These policies should be consistently communicated in languages other than English, when needed, based on the languages spoken in the community, to avoid marginalization of parents/guardians of limited English proficiency or who do not speak English.
Ongoing federal, state, and local funding should be provided for all schools so they can continue to implement all the COVID-19 mitigation and safety measures required to protect students and staff. Funding to support virtual learning and provide needed resources should continue to be available for communities, schools, and children facing limitations implementing these learning modalities in their home (eg, socioeconomic disadvantages) or in the event of school re-closure because of a resurgence of SARS-CoV-2 in the community or a school outbreak.
With the above principles in mind, the AAP strongly advocates that all policy considerations for school COVID-19 plans should start with a goal of keeping students safe and physically present in school. The importance of in-person learning is well-documented, and there is already evidence of the negative impacts on children because of school closures in 2020.13
Policy makers and school administrators must also consider the scientific evidence regarding COVID-19 in children and adolescents, including the role they may play in the transmission of the infection. 14,15,16,17,18,19,20,21,22Although many questions remain, the preponderance of evidence indicates that children and adolescents are less likely to have severe disease resulting from SARS-CoV-2 infection. 23,24 We continue to learn more about the role children play in the transmission of SARS-CoV-2. At present, it appears that children younger than 10 years are less likely to become infected and less likely to spread the infection to others, although further studies are needed. 25,26,27 Some data suggest children older than 10 years may spread SARS-CoV-2 as efficiently as adults. Additional in-depth studies are needed to truly understand the infectivity and transmissibility of this virus in anyone younger than 18 years, including children and adolescents with disabilities and medical complexities. Current SARS-CoV-2 variants may change both transmissibility and infection in children and adolescents even in those who have been vaccinated.
Visit the CDC COVID-19 Prevention Strategies for additional information on mitigation measures including physical distancing, testing, contact tracing, ventilation, and cleaning and disinfecting.
In the following sections, some general principles are reviewed that policy makers and school administrators should consider as they safely plan for in-person school. There are several other documents released by the CDC, the National Association of School Nurses, and the National Academy of Sciences, Engineering, and Medicine that can be referenced as well. For all of these, engagement of the entire school community, including families, teachers, and staff, regarding these measures should be a priority.
Special Considerations for School Health During the COVID-19 Pandemic
School Attendance and Absenteeism: Studies performed throughout the pandemic demonstrated wide variability in tracking of school attendance. As of January 2021, only 31 states and the District of Columbia required attendance to be taken.28 Definitions of attendance for individuals participating in distance learning have varied between and within states. Among jurisdictions that did report on attendance during the pandemic period, several studies demonstrate disparities in impact of chronic absence.29 In an evaluation of Connecticut’s attendance data from school year 2020-21, rates of chronic absenteeism were highest among predominantly remote students compared with students who were primarily in-person; that gap was most pronounced among elementary and middle school students. Chronic absence was more prevalent among Connecticut students who received free or reduced-price lunch, were Black or Hispanic, were male, or identified as English learners or having disabilities.29 National prepandemic chronic absenteeism data mirror several of these demographic trends.30
The best way to reduce absenteeism is by closely monitoring attendance and acting quickly once a pattern is noticed.31 During the the 2021-22 school year, daily school attendance should be monitored for all students; for students participating in in-person and distance learning. Schools should use multi-tiered strategies to proactively support student attendance for all students. Additionally, schools should implement strategies to identify and differentiate interventions to support those at higher risk for absenteeism. Local data should be used to define priority groups whose attendance has been most deeply impacted during the pandemic. Schools are encouraged to create an attendance action plan with a central emphasis on family engagement leading up to and through the start of school.
With the beginning of the 2021-22 school year, plans should be in place for outreach to families whose students do not return for various reasons. This outreach is especially critical, given the high likelihood of separation anxiety and agoraphobia in students. Students may have difficulty with the social and emotional aspects of transitioning back into the school setting, especially given the unfamiliarity with the changed school environment and experience. Special considerations are warranted for students with pre-existing anxiety, depression, and other mental health conditions; children with a prior history of trauma or loss; children with autism spectrum disorder; and students in early education who may be particularly sensitive to disruptions in routine and caregivers. Students facing other challenges, such as poverty, food insecurity, and homelessness, and those subjected to ongoing inequities may benefit from additional support and assistance. Schools should identify students who are at risk for not returning and conduct outreach prior to the beginning of the school year. Resources should be available to assist families with preparing their student for transition back to school.
Students with Disabilities: The impact of loss of instructional time and related services, including mental health services, as well as occupational, physical, and speech/language therapy during the period of school closures and remote learning is significant for students with disabilities. All students, but especially those with disabilities, may have more difficulty with the social and emotional aspects of transitioning out of and back into the school setting because of the pandemic. As schools prepare for or continue in-person learning, school personnel should develop a plan to ensure a review of each child and adolescent with an IEP to determine the needs for compensatory education to adjust for lost instructional time and disruption in other related services. In addition, schools can expect a backlog in evaluations; therefore, plans to prioritize students requiring new referrals as opposed to reviews and re-evaluations will be important. Many school districts require adequate instructional effort before determining eligibility for special education services. However, virtual instruction or lack of instruction should not be reasons to avoid starting services such as response-to-intervention (RTI) services, even if a final eligibility determination is delayed.
Each student’s IEP should be reviewed with the parent/guardian/adolescent yearly (or more frequently if indicated). All recommendations in the IEP should be provided for the individual child no matter which school option is chosen (in person, blended, or remote). See the AAP Caring for Children and Youth with Special Health Care Needs During the COVID-19 Pandemic for more details.
Additional COVID-19 safety measures for teachers and staff working with some students with disabilities may need to be in place to ensure optimal safety for all. For certain populations, the use of face masks by teachers may impede the education process. These include students who are deaf or hard of hearing, students receiving speech/language services, young students in early education programs, and English language learners. There are products (eg, face coverings with clear panels in the front) that may be helpful to use in this setting.
Adult Staff and Educators: Universal use of face masks is recommended, given that certain teachers must cross-over to multiple classes, such as specials teachers, special educators, and secondary school teachers, and in consideration of new SARS-CoV-2 variants. At this time, this recommendation for use of face masks includes staff and educators who have been fully vaccinated, especially for teachers with students who are unvaccinated (including pre-K, kindergarten, and elementary schools). School staff working with students who are unable to wear a face mask or who are unable to manage secretions, who require high-touch (hand over hand) instruction, and who must be in close proximity to these students should consider wearing a surgical mask in combination with a face shield.
School health staff should be provided with appropriate medical PPE to use in health suites. This PPE should include N95 masks, surgical masks, gloves, disposable gowns, and face shields or other eye protection. School health staff should be aware of CDC guidance on infection control measures.
On-site School-Based Health Services: On-site school health services, including school-based health centers, should be supported if available, to complement the pediatric medical home and to provide pediatric acute, chronic, and preventive care. Collaboration with school nurses is essential, and school districts should involve school health services staff and consider collaborative strategies that address and prioritize immunizations and other needed health services for students, including behavioral health, vision screening, hearing, dental and reproductive health services. Plans should include required outreach to connect students to on-site services regardless of remote or in-person learning mode.
Immunizations: Pediatricians should work with schools and local public health authorities to promote childhood vaccination messaging well before the start of the school year and throughout the school year. It is vital that all children receive recommended vaccinations on time and get caught up if they are behind as a result of the pandemic. The capacity of the health care system to support increased demand for vaccinations should be addressed through a multifaceted, collaborative, and coordinated approach among all child-serving agencies including schools.
Existing school immunization requirements should be discussed with the student and parent community and maintained. In addition, although influenza vaccination is generally not required for school attendance, it should be highly encouraged for all students and staff. The symptoms of influenza and SARS-CoV-2 infection are similar, and taking steps to prevent influenza will decrease the incidence of disease in schools and the related lost educational time and resources needed to handle such situations by school personnel and families. School districts should consider requiring influenza vaccination for all staff members.
Schools should collaborate with state and local public health agencies to ensure that teachers and staff have access to the COVID-19 vaccine and that any hesitancy is addressed as recommended by the Advisory Committee on Immunization Practices (ACIP) of the CDC. Pediatricians should work with families, schools, and public health to promote receipt of the COVID-19 vaccine and address hesitancy as the vaccine becomes available to children and adolescents.
In order to vaccinate as many school staff, students, and community members as possible, school-located vaccination clinics should be a priority for school districts. Schools are important parts of neighborhoods and communities and serve as locations for community members after school hours and on weekends.
Vision Screening: Vision screening practices should continue in school whenever possible. Vision screening serves to identify children who may otherwise have no outward symptoms of blurred vision or subtle ocular abnormalities that, if untreated, may lead to permanent vision loss or impaired academic performance in school. Personal prevention practices and environmental cleaning and disinfection are important principles to follow during vision screening, along with any additional guidelines from local health authorities.
Hearing Screening: Safe hearing screening practices should continue in schools whenever possible. School screening programs for hearing are critical in identifying children who have hearing loss as soon as possible so that reversible causes can be treated and hearing restored. Children with permanent or progressive hearing loss will be habilitated with hearing aids to prevent impaired academic performance in the future. Personal prevention practices and environmental cleaning and disinfection are important principles to follow during hearing screening, along with any additional guidelines from local health authorities.
Children with Chronic Illness: Certain children with chronic illness may be at risk for hospitalization and complications with SARS-CoV-2. These youth and their families should work closely with their pediatrician and school staff using a shared decision-making approach regarding options regarding return to school, whether in person, blended, or remote. See the AAP Caring for Children and Youth with Special Health Care Needs During the COVID-19 Pandemic for more details.
Behavioral Health/Emotional Support for Children and Adolescents: The COVID-19 pandemic has created profound challenges for communities, families, and individuals, leading to a range of emotional and behavioral responses. There are many factors unique to this pandemic (eg, grief/loss, uncertainty, rapidly changing and conflicting messages, duration of the crisis, and need for quarantine) that increase its effects on emotional and behavioral health (EBH). Populations with a higher baseline risk, such as historically under-resourced communities, children and youth with developmental disabilities and other special health care needs, may be especially vulnerable to these effects. 32,33 The impact of the pandemic is also compounded by isolation and an interruption in the support systems families utilize.
Schools are a vital resource to continue to address and provide resources for a wide range of mental health needs of children and staff. The emotional impact of the pandemic, grief because of loss, financial/employment concerns, social isolation, and growing concerns about systemic racial inequity—coupled with prolonged limited access to critical school-based mental health services and the support and assistance of school professionals—demand careful attention and supports in place during all modes of learning, whether remote or in-person. Schools should be prepared to adopt an approach for mental health support, and just like other areas, supporting mental health will require additional funding to ensure adequate staffing and the training of those staff to address the needs of the students and staff in the schools.
Schools should consider providing training to classroom teachers and other educators on how to talk to and support children during and after the COVID-19 pandemic including how to support grief and loss among students. The United States has already accumulated more than 600,000 deaths from COVID-19; on average, it is estimated that each of these deaths impacts 9 people – many of these 4.5 million grieving individuals are children. Bereavement has a significant impact on the short- and long-term adjustment of children, their developmental trajectory, academic learning, psychosocial functioning, and emotional adjustment and behavior. Students experiencing significant personal losses can be referred to school and community-based bereavement support programs, centers, and camps, as well as to their pediatrician or other pediatric health care provider.34 Students with additional mental health concerns should be referred to school mental health professionals.
Suicide is the second leading cause of death among adolescents or youth 10 to 24 years of age in the United States.35 Schools should develop mechanisms to evaluate youth remotely and in-person if concerns about a risk of suicide are voiced by educators or family members and should be establishing policies, including referral mechanisms for students believed to be in need of in-person evaluation, even before schools resume in-person instruction.
School mental health professionals should be involved in shaping messages to students and families about the response to the pandemic and the changing school learning plans based on a variety of community SARS-CoV-2 factors. Fear-based messages widely used to encourage strict physical distancing may cause problems when schools resume in-person instruction, because the risk of exposure to COVID-19 may be mitigated but not eliminated. Communicating effectively is especially critical, given potential adaptations in plans for in-person or distance learning that need to occur during the school year because of changes in community transmission of SARS-CoV-2.
Schools need to incorporate academic accommodations and supports for all students who may still be having difficulty concentrating or learning new information because of stress or family situations that are compounded by the pandemic. It is important that school personnel do not anticipate or attempt to catch up for lost academic time through accelerating curriculum delivery at a time when students and educators may find it difficult to even return to baseline rates. These expectations should be communicated to educators, students, and family members so that school does not become a source of further distress
The personal impact on educators and other school staff should be recognized. In the same way that students need ongoing support to process the information they are being taught, teachers cannot be expected to be successful at teaching children without having their mental health needs supported. The strain on teachers, as they have been asked to teach differently while they support their own needs and those of their families, has been significant. Additional challenges with staff shortages, changing learning modalities, and prolonged duration of the crisis are continuing to present additional challenges and further impact teachers and school staff. Resources such as Employee Assistance Programs and other means to provide support and mental health services should be prioritized. The individual needs and concerns of school professionals should be addressed with accommodations made as needed.
Although schools should be prepared to be agile to meet evolving needs and respond to increasing knowledge related to the pandemic and may need to institute partial or complete closures when the public health need requires, school leaders should recognize that staff, in addition to students and families, will benefit from sufficient time to understand and adjust to changes in routine and practices. During a crisis, people benefit from clear and regular communication from a trusted source of information and the opportunity to dialogue about concerns and needs and feel they are able to contribute in some way to the decision-making process. Change is more difficult in the context of crisis and when predictability is already severely compromised.
Food Insecurity: According to the United States Department of Agriculture, the number of food-insecure households has increased during the pandemic with a currently estimated 30 million adults and 12 million children living in households where they may not get enough to eat.36 We also know that disparities with food insecurity exist, with Black and Latino adults being twice as likely as white adults to report their households did not get enough to eat.34School planning must consider the many children and adolescents who experience food insecurity already (especially at-risk populations and those living in poverty) and those who will have limited access to routine meals through the school district in the event of school closure or if a child is ill. The short- and long-term effects of food insecurity in children and adolescents are profound.37 Schools can partner with community resources including federal and state food programs to mitigate the effects of food insecurity on children and families. More information about how families can access federal nutrition programs can be found in the AAP/FRAC Food Insecurity Toolkit.
Housing Insecurity: Like food insecurity, housing insecurity is a significant and sometimes overlooked issue that affects many families and will impact children’s ability to return and re-engage with school. With pandemic-associated job losses, there have been significant numbers of families with children who have been evicted or will soon be evicted from their homes. According to the US Census Bureau, as of February 2021, there are 5.2 million households with children who are behind on rent and 4.5 million homeowners with children behind on mortgage payments.38 Housing insecurity impacts a child’s education directly through missed school days and through transferring to a new school, which is associated with a 4 times higher risk of chronic absenteeism, lower grades and test scores, and increased risk of dropping out of school.39 Housing insecurity also impacts education indirectly by impacting a child’s overall physical and mental health, which can have negative consequences for educational achievement. Children who experience homelessness are at increased risk for malnutrition, asthma, obesity, and dental, vision, emotional, behavioral, and developmental problems.40 In addition, the increased toxic stress children experience when they live in unstable housing situations can contribute to anxiety and other mental health conditions that interfere with a child’s education. The interconnectedness of employment, housing, health, and education and the disproportionate impact this has had on communities of color because of structural racism must be considered as children return to school.41 Schools are encouraged to partner with community agencies to address the effects of housing insecurity and mitigate the impact this will have on the education of children.
Digital Divide: The digital divide has been a known disparity for decades, contributing to the “homework gap”—the gap between school-aged children who have access to high-speed internet at home and those who do not. According to a Pew research study in 2015, 35% of lower-income households with school-aged children did not have a broadband internet connection at home. According to the Pew Research Center, 1 in 5 teenagers are not able to complete schoolwork at home because of a lack of a computer or internet connection.42 This technological homework gap disproportionately affects Black families living in poverty.9 With the transition to virtual learning during the pandemic, this divide was highlighted as families struggled to adapt to school from home. In April 2020, 59% of parents with lower incomes who had children in schools that were remote because of the pandemic said their children would likely face at least 1 of 3 digital obstacles to their schooling, such as a lack of reliable internet at home, no computer at home, or needing to use a smartphone to complete schoolwork. Gains have been made over this past year with creative local and state solutions working toward providing improved access to both technology devices and internet connections for students, but a significant gap still exists, particularly for students living in poverty. This digital divide is a critical component to be addressed in schools even as children return to in-person learning as they navigate the increasing digital learning environment, academic recovery, and extended home learning materials. Access to both reliable high-speed internet and adequate devices beyond a smart phone are critical to promote equity and support academic success.Long-term sustainable funding is needed to support school districts in providing universal internet access and technology for all students.
Organized Activities: It is likely that sporting events, practices, and conditioning sessions as well as other extracurricular activities will be limited in some locations while reopening fully in other locations. The AAP Interim Guidance on Return to Sports helps pediatricians inform families on how best to ensure safety when considering a return to sports and physical activity participation. Preparticipation evaluations should be conducted in alignment with the AAP Preparticipation Physical Evaluation Monograph, 5th ed, and state and local guidance.
The Ohio Department of Health released updated recommendations for K-12 schools yesterday. The guidance strongly recommends COVID-19 vaccinations for staff and eligible students; consistent…
The Centers for Disease Control issued new guidance Tuesday for back to school protocol.
Rochelle P. Walensky, MD, MPH, Director, Centers for Disease Control and Prevention said in a news conference that new scientific data from recent outbreak investigations show the Delta Covid-19 variation is uniquely, differently from past strains of the virus. Even those who are fully vaccinated may become contagious and spread the Delta variant to others.
Walensky recommended:
1) Everyone should get vaccinated and continue masking until fully vaccinated. In high transmission areas of the country, vaccinated individuals should wear masks indoors. This includes schools.
2) Everyone in K-12 schools wears a mask indoors including students, teachers, staff, and visitors regardless of vaccination status.
3) Children should return to full-time/in-person learning in the Fall with proper prevention strategies in place.
4) Community leaders should encourage vaccination and universal masking to prevent further outbreaks in areas of substantial and high transmission.
EDITOR’S NOTE: This story was updated 6:55 AM 7-29 to reflect that Loveland Schools will return to full in-person learning in August.
Loveland, Ohio – Below is the face covering and mask requirements for the current school year in Loveland schools. This policy was adopted by the Board of Education on June 3, 2021.
There will be no remote learning opportunities for teachers or students as all school buildings will return to full capacity in-person classes in August. The District announced on May 7 that, “Due to a lack of interest from our families, Loveland City School District will not be offering the Remote Academy for the 2021-2022 school year. We look forward to welcoming back all of our students for five-day per week in-person learning in the fall!”
Revised June 3, 2021
8450.01 – USE OF FACE COVERINGS/MASKS
The Loveland Board of Education is committed to providing students, staff, and visitors with a safe and healthy environment.
On May 12, 2021, Ohio Governor Mike DeWine lifted the State’s COVID – 19 mask requirements, including the requirement of face coverings inside public buildings, effective June 2, 2021 Furthermore, he declared that local school districts will make their own determinations on Covid-19 mitigation efforts, including the wearing of masks and/or face shields.
As of the adoption date, June 3, 2021, of this updated policy, unless required by additional mandates, the decision to wear face coverings/masks on school buses, in school buildings, or at other school events, will be left to adult individuals and parents/guardians of K-12 students. The Loveland City Schools will continue to follow COVID-19 mitigation protocols to maintain a healthy environment for students, staff, and visitors and will continue to provide recommendations for personal protection from the spread of infectious diseases.¶
In order to maintain a healthy environment, the Board will follow any mandates set forth by the Ohio Governor, Ohio State Health Department, Hamilton County Health Department, and Ohio Department of Education, (“Directing Entities”) as it relates to protecting the health of students, staff and visitors. When any of these Directing Entities requires staff, students, and visitors to wear face coverings/masks while attending school, reporting to work at a school, or visiting a school, the District’s Administration will follow and enforce such directives.