“As we begin the process of redetermining eligibility for the first time in three years, we must pay particular attention to children’s needs to minimize the number of children who lose coverage.”
A new study warns of a sharp rise in uninsured children in Ohio and across the country if pandemic-era coverage is allowed to fade away.
The Georgetown University Health Policy Institute’s Center for Children and Families studied the impact of the Children’s Health Insurance Program (CHIP) and Medicaid on bringing down state’s uninsured rate, finding that it “proved to be a critical lifeline for more than half of the nation’s children during the pandemic.”
Now that a March 2020 provision increasing the federal contribution to state Medicaid programs while requiring states to maintain continuous coverage for Medicaid patients during the COVID-19 public health emergency will be going away, the number of children falling under those protections will also be decreasing.
“These children are at grave risk of losing coverage inappropriately in states that do not handle the renewal process with the utmost care,” the study stated.
Because of a loss of income eligibility and “bureaucratic snafus,” the study estimates up to 6.7 million children in the U.S. will lose coverage because of the “unwinding” of pandemic-era programs, scheduled to happen on April 1.
“The uninsured rate for children could easily more than double if states have inadequate staffing levels and overwhelmed call centers and do not take the time and care needed to properly conduct eligibility checks after the federal protections lift,” the study stated.
From February 2020 to August 2022, Ohio saw a 26.7% increase in Medicaid and CHIP enrollment, ranking them 29th in the nation based on data from the Centers for Medicare & Medicaid Services. The share of enrollment made up by children in Ohio was 25.6%.
“As we begin the process of redetermining eligibility for the first time in three years, we must pay particular attention to children’s needs to minimize the number of children who lose coverage,” Kelly Vyzral, senior health policy associate for the Children’s Defense Fund-Ohio, said in response to the study.
The Children’s Defense Fund-Ohio said nearly half of children in Ohio are covered by Medicaid and other public health insurance programs. The study showed 54% of all American children are covered by Medicaid of CHIP.
Ohio already has the 12-month continuous Medicaid and CHIP child eligibility for those under age 19 recommended by the study to mitigate losses and gaps in coverage.
Continuous eligibility protects parents who see an increase in income during a 12-month period from losing child Medicaid or CHIP coverage.
Ohioans should verify contact information with local benefits offices or through the Medicaid patient portal to avoid cancellation of child insurance, Vyzral said.
Ohio must complete Medicaid eligibility checks by May 2024.
The Plain City Public Library asked her to leave in January 2021 for repeatedly refusing to wear her mask, as was state policy at the time.
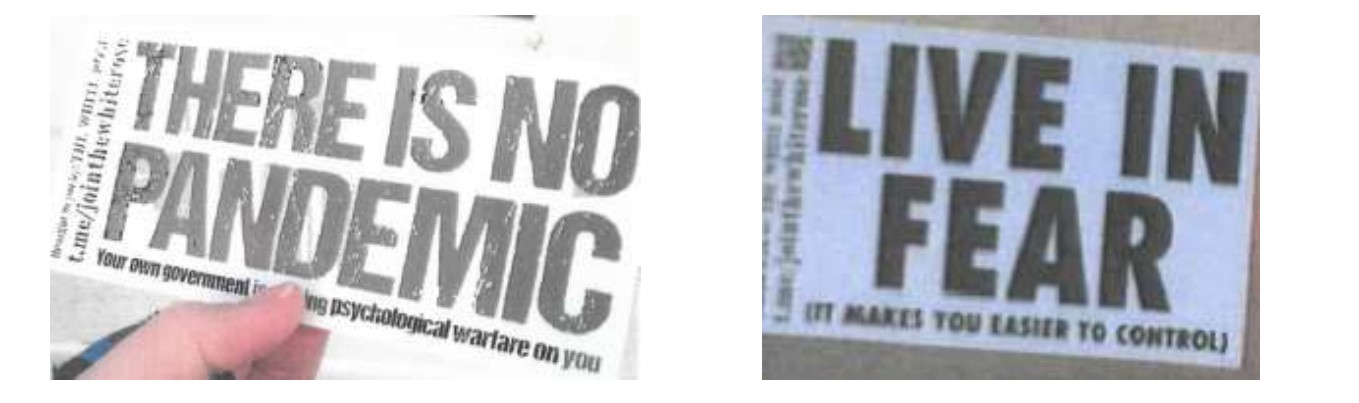
Court records indicate Julie Dean’s “unruly behavior had been a continual issue for the library.” Two months later she came back with her husband and some hard-to-remove stickers.
“THERE IS NO PANDEMIC,” reads the first one. “Your own government is waging psychological warfare on you.”
“LIVE IN FEAR,” reads the other. “(It makes you easier to control.)”
Julie and Samuel Dean were subsequently accused and convicted of misdemeanor criminal charges of trespassing and criminal mischief. Their case set off a bizarre bout of trials and appeals that distill some of the anger and paranoia that continues to dog the coronavirus pandemic.
Their case, which led to a $250 fine and two-day prison sentence, is now pending with the Ohio Supreme Court. The stickers, placed on a library drop box installed during the pandemic, have since only been partially removed.
After the court appointed the Deans an attorney, the couple fired him and chose to represent themselves. They soon filed near-identical motions a judge found nearly impossible to decipher but mentioned an objection to “undertake a medical intervention without any informed consent and without any medical necessity.”
In a pre-trial hearing, Samuel Dean asked that the court dismiss the charges against him, claiming in prepared remarks that his rights under the Americans With Disabilities Act were violated. However, court records state he repeatedly “refused” to say what kind of accommodations he sought. When a judge said he can’t help if he doesn’t know how, Samuel Dean read the same prepared statement again.
“That does nothing for me,” the judge said.
He later found Samuel Dean in contempt for talking over him and fined him $250. The judge then called Julie Dean’s case. She then read the same prepared remarks as her husband before telling the judge that he had “been served.”
“Well, I haven’t,” the judge responded before setting the matter for trial.
The deans then both filed affidavits with the Ohio Supreme Court seeking to disqualify the judge from their case. Those were denied.
The case then went to trial. The Deans acted as their own attorneys. After 20 minutes of deliberation, a jury found each of them guilty on two counts. They each received a $250 fine and 90 days in jail, but they only needed to serve two. They haven’t yet served those sentences.
The trespassing charge against Samuel Dean was dismissed on appeal earlier this month. Judge Stephen Powell of the Twelfth Appellate District found that because he hadn’t been previously banned from the library, he wasn’t trespassing. (A dissenting judge argued his criminal intent to deface the library should have waived his privilege to be on its property.)
On Monday, the Deans appealed their case to the Ohio Supreme Court. L. Bradfield Hughes, an attorney with Porter, Wright, Morris and Arthur, said in court filings that the case raised “questions of public and great general interest.”
They argued they have been improperly denied the use of an ADA coordinator at lower court proceedings. An attorney with the Madison County Prosecuting Attorneys office denied this, noting that both state and federal courts who reviewed the matter ruled there has been no such violation. In the related federal lawsuit, Julie Dean claimed she suffers from hearing and memory loss. Samuel Dean said he suffers PTSD. These disabilities, they said, “substantially limit their life activities” and were ignored by the court. The claims were dismissed.
Attorneys for both sides didn’t respond to phone calls.
Chris Long, director of the library, said in an interview that it’s easy to focus on the loudest blips on the radar. But far more prevalent are ordinary bookworms staying positive in a difficult era.
“Public libraries, we see a lot everyday, pandemic and no,” she said. “For every difficult situation, we encounter dozens more of people wanting to help.”
As nurses, my husband and I witnessed truly awful and devastating things treating patients on the frontlines of this pandemic. Hundreds of thousands of Americans have died, while the millions who survived, now faced with disability, are left to grapple with the harsh realities of long COVID-19.
Among those millions of people living with long-term health impacts is our son Carter.
Four days before the COVID-19 vaccine was available for kids under 12, my 11-year-old son Carter tested positive for COVID-19. He had the common symptoms for the first few days, but as those subsided, I began noticing new ones like extreme thirst and frequent urination. In my gut, I knew it was diabetes. And sure enough, a mother always knows: Twelve days after his COVID-positive test, Carter was officially diagnosed with Type 1 diabetes.
In less than a month, everything about our lives changed. We don’t have any family history of any type of diabetes, so Carter’s diagnosis came out of nowhere, and we were not prepared. Our days now revolve around his blood sugar levels. Meal times are planned around insulin doses, mornings and evenings have a new medicine routine. Even as nurses, my husband and I could have never anticipated the severity of impact this diagnosis would have on our family.
I hear fellow nurses say there are more kids coming into the hospital and leaving with a diabetes diagnosis. Many of the newly diagnosed diabetics often had a recent COVID-19 infection. When a recent CDC report found children under 18 infected with COVID-19 are 2.66 times more likely to develop diabetes, it only confirmed the trend I witnessed in my hospital.
Carter was prescribed two different kinds of insulin, Humalog and Basaglar. Only a couple months into his treatment, our insurance decided it would no longer cover Humalog beginning in January of this year. We had just enough to last us through March. We cannot afford the out-of-pocket costs to keep Carter on the same kind of insulin, so we will need to switch him to a new kind of insulin before his body has even adapted to the current regimen.
We lose sight of the human cost when we ignore insulin price gouging. At the end of the day, we are putting a price on human life — on a child’s life.
I realize we are extremely lucky to have health insurance that keeps insulin costs manageable for our family. Since becoming part of the diabetes community, I’ve learned how rare it is to have sufficient insurance coverage and be able to afford insulin at all. As I read the heart-breaking posts from parents pleading for insulin donations in online communities, I think about how one unfortunate diagnosis can send a family to economic ruin through no fault of their own.
So, when the House passed the Affordable Insulin Now Act last week, I felt like Congress finally listened to the pleas of Americans with diabetes. The bill will cap insulin copays at $35 a month — reducing insulin costs by hundreds each year. In America, around 1 in 4 diabetics have rationed their insulin due to high costs. With nearly 60% of Americans under 17 having been infected with COVID-19, some of them may develop type 1 diabetes. It is more important than ever to do something about insulin prices.
By lowering the price of insulin and passing other federal prescription drug reforms, we can help existing diabetics and prevent newly diagnosed diabetics, especially kids, from being forced to ration life-saving medication.
I couldn’t imagine going through this emotional journey with the added stress of not being able to afford the one thing you need to keep your child alive. Type 1 diabetes is a lifelong condition; my son will never escape this. It’s not his fault he caught COVID-19. It’s not his fault that COVID-19 may have caused his diabetes. But he will be forever burdened by the price of insulin.
We are fortunate to be able to afford Carter’s insulin and supplies. But what about the families who aren’t so lucky? What happens to all of the kids who will eventually age off of their parents’ insurance, and their plans barely cover insulin? We lose sight of the human cost when we ignore insulin price gouging. At the end of the day, we are putting a price on human life — on a child’s life.
I would do whatever I could to get my child what he needs. I would give up my house, I would give up everything to keep him alive. I don’t know any parent who wouldn’t do the same. Our leaders in Congress must do everything they can, so people with diabetes and their caretakers aren’t left with such impossible choices. Now, it’s up to our representatives in the Senate to stand with parents like me and stop hiding behind the donations of pharmaceutical companies.
This commentary was first published in the Arizona Mirror.
The last thing people want to hear right now is that the coronavirus might have mutated yet again into yet another deadly variant, extending the pain, death, and inconvenience of a pandemic that we long hoped would be over.
However, whether the subvariant of omicron known as BA.2 will hit the United States as hard as it’s hitting other parts of the world is hard to say at this point, an expert at modeling the disease said Wednesday.
The pandemic has been full of unpleasant surprises and BA.2 is no exception. Scientists estimate that it’s one-and-a-half times as transmissible as the original omicron strain, BA.1, and is overtaking it.
Europe, and particularly the United Kingdom, have seen an increase in the new variant in recent months, but that hasn’t been the case everywhere, said Stephen Kissler, a research fellow in the Department of Immunology and Infectious Diseases of Harvard University’s T.H. Chan School of Public Health.
“The question of if and when a surge is coming and how large is very open,” Kissler said in a Zoom conference with reporters. “I know that we’ve seen surges that are dominated by BA.2 across much of Europe. But in contrast, for example, in South Africa we saw a major BA.1 wave — that’s where we saw the omicron wave first — and now there’s a lot of circulation of BA.2, but it hasn’t really caused an increase in cases so much that it’s lengthened the decline and given the epidemic a very long tail.”
Kissler explained that vaccination rates in the U.S. are lower than those in Europe, but higher than those in South Africa. That could mean that more Americans have developed antibodies against the omicron variants than have Europeans.
“To the extent that that gives us protection against BA.2 we might see dynamics that are more similar to what happened in South Africa,” he said.
Seasonality and other factors likely will play a role, Kissler said, with spring in the United States being a season of relatively low spread and fall a season of relatively high spread.
So if there is a surge here of the new variant, how will it affect Americans of varying ages?
“In many ways it will likely resemble our experience with COVID-19 up to this point,” Kissler said.
And past experience has shown one factor to be hugely important: vaccination.
Kissler said that being vaccinated, along with a booster dose, “really goes a long way toward helping to protect you from symptomatic disease and especially severe disease. The biggest delineation I imagine seeing is that people who are boosted will probably fare better than people who are unboosted.”
Another important factor is age, with the elderly having less natural resistance to all variants of the coronavirus than the young. Vaccines and boosters, though, can be a great equalizer.
“A vaccinated and boosted person over the age of 75, their risk is probably on the order of — if not lower than — an unvaccinated 20-year-old,” Kissler said.
COVID eventually will go from being a pandemic disease that spikes rapidly and overwhelms resources to an endemic one where a background level is present, sickening and even killing people, but in semi-predictable ways. Sadly, however, hopes that it will disappear altogether are small.
Looking forward, one simple public-health measure might be most effective, Kissler said.
“In many ways, one of the best things we can do to manage outbreaks is to just to continue to keep informing people how much COVID is circulating in their communities and make it just as accessible as a weather report,” he said. “A lot of data suggest that people tend to adjust their behavior accordingly.”
He said that probably won’t be enough to quell future waves of COVID, or be adequate in the face of major new variants.
“But as we continue to deal with COVID and we think about this permanent circulation of COVID-19 in the population — recognizing that there’s going to be different dynamics in different places, different patterns across the year — making it clear what’s happening in any given community at any given time through passive surveillance is probably the best thing we can do right now,” he said.
JANUARY 10, 2022
It’s been a tough couple of years for everyone – adults and kids alike.
When the pandemic first started, we were all worried about getting the illness. That sentiment certainly still exists for some, in particular people who are immunocompromised and the elderly. However, it seems we have now transitioned into a more generalized anxiety related to COVID-19, but not necessarily about contracting it. And the unfortunate reality is that our kids are feeling the same way.
THE SITUATION: MORE KIDS HAVE ANXIETY NATIONWIDE
We’re seeing more kids with anxiety nationwide. More psychology visits. More visits to the Emergency Department for suicide attempts. In fact, suicide is the second-leading cause of death in kids 10 years and older.
I don’t mention this to cause panic in parents, but rather to heighten our sense of awareness. Our kids have suffered much in the way that adults have, and we need to watch and take note (more on that later). While we don’t have an exact link to causation at this time, we certainly can make some guesses.
WHY KIDS HAVE COVID-RELATED ANXIETYWe’re noticing that kids are behaving in ways that are similar to how we act after experiencing significant loss. And I think this makes sense. They have missed out on nearly two years of normalcy. Two years of attending school in a typical way. Two years of uncertainty and disbelief. They’ve missed major milestones and activities, such as graduation, school dances, field trips and sporting events.
Not to mention the developmental impacts of virtual school. Kids learn by interacting with others and through hands-on projects. They develop socially by having to navigate relationships and work things out. Their sense of well-being, especially for teens, is tied to their peers and achievements. And now that some of these activities have started up again, many are anxious about returning to them, because they’re out of practice.
So what can we as parents do about it? I recommend the following:
1. ENCOURAGE RESILIENCYResiliency is the ability to manage and bounce back from a stressor. Without social interactions and activities, these skills have been sitting on a shelf. They need to be dusted off and used. This will take work and time. It can start by explaining that they have the ability to do it – they can do hard things. Perhaps remind them of another time when they worked through something difficult. Have them focus on what’s within their control and let go of what isn’t. Read this previous post for more tips on teaching resiliency.
2. PROMOTE BASIC BRAIN HEALTHThe last couple of years have wreaked havoc on our basic brain health, and this impacts how we think and feel. We’ve gotten out of our normal routines, sleeping patterns and healthy meals. I recommend getting back to a daily structure. Have a normal bedtime. Engage in regular physical activity. Eat meals together. It doesn’t have to be every day or even at dinner, but children who eat meals with their families are often more resilient than those who don’t eat with their family.
3. NURTURE PARENT-CHILD CONNECTIONSConveying a sense of connection with your children is so important for their sense of well-being and willingness to open up to us. Just hang out together and have fun on a consistent basis. You don’t have to have big important discussions. This will plant the seed for them to trust you and confide in you when they need help.
4. TAKE CARE OF YOURSELFThis goes back to the oxygen mask metaphor – when you’re on a plane, you need to put your oxygen mask on before you help someone else put theirs on. The same goes for mental health. It is difficult to help someone else when you’re not taking care of yourself. I realize this is easier said than done, but start taking small steps. Ask another adult to partner with you in making self-care a priority.
5. NOTICE CHANGES IN YOUR CHILDBasic changes in your children can indicate that they are having a difficult time. Be on the lookout for changes in sleep, eating, appearance, academics, energy level, activities, and social interactions. Pay attention to their social media accounts. When you notice any of these differences, ask them about it. Say something like, “I’ve noticed you’re eating less than normal”. Or, “you’re not hanging out with Suzie as much”. Follow up with, “let’s talk about that”. Or, “have you noticed that too”? They may not be open up right at that moment, but you’ve opened the door and it may lead to more conversations. And if you’re concerned, say so.
6. GET HELP WHEN NEEDEDIt is okay to ask if they’ve had thoughts of suicide or wanting to die. Parents sometimes worry that they will plant those thoughts in their heads, but this just isn’t the case. This allows them to share concerning thoughts with us. By asking difficult questions, parents open the door for children to discuss difficult topics. Children who talk about these feelings with trusted adults are at less risk of acting on them.
If you notice significant changes in your children, or if they talk about wishing they were dead or having thoughts of killing themselves, never hesitate to contact a professional. You can reach out to our Pediatric Intake Response Center at 513-636-4124, our Division of Behavioral Medicine and Clinical Psychology at 513-636-8107, or refer to a list of contacts on our mental health and resources page.
Loveland, Ohio – Loveland parents Leah Marcus and Becca Moates say, “Hey all, It’s time to take our combined effort and show our Superintendent and School Board what is important.” They wrote a template letter, a petition, with the help of who they call a super IT friend to solicit support to help them protect school children, teachers, and the community by performing the following COVID 19 related steps.
Copy the contents of the below template and paste it into the body of the email message.
Add your name and additilal comment to the bottom of the document.
Share your voice by hitting send.
Moates adds, “I can’t stress enough how important it is as a community for us to come together around this. Our healthcare systems are drowning and we are hurting our most vulnerable if we don’t act.”
Dear Superintendent and School Board Members,
I am writing as a resident of the Loveland City School District to urge you, our Superintendent and elected School Board members, to maintain the all staff and PreK through 6th grade universal indoor masking requirements, scheduled to end January 18, 2021. I am also writing to request that the current universal indoor masking requirement be expanded to include students in grades 7 -12.
This request is being made in consideration of the recent COVID-19 Omicron variant case surge, which has been shown to be more transmissible and contagious than previous variants.
The Ohio Department of Health, the Ohio Department of Education, the American Academy of Pediatrics, the CDC, and locally, the Cincinnati Children’s Hospital Medical Center, recently provided clear guidance for universal masking in schools and in the community. Universal indoor masking, in addition to vaccination and boosters for those eligible, are strongly recommended as the best tools, especially when used in tandem, for mitigating the spread of COVID-19 and the current variant.
The pandemic also continues to take a toll on our children’s and educators’ mental health. Since the pandemic began, rates of psychological distress among young people, including anxiety, depression, and other mental health disorders have increased substantially. There is much to be done and each of us has a part to play. Supporting the mental health of youth will require a community effort to address challenges, strengthen the resilience of young people, support their families, and mitigate the pandemic’s mental health impact.
As a resident of the Loveland City School District, I am asking that you consider the following actions:
1. Maintain universal indoor masking for all staff.
2. Maintain Universal indoor masking for all students Pre-K through Grade 6.
3. Expand universal indoor masking requirements to include students in grades 7 - 12.
4. Identify a threshold for educator and/or student absence at which the district will move forward with a remote learning plan.
5. Increase the frequency with which you report to the public student and educator absences as well as individuals positive for COVID.
6. Create and promote safe, positive, and affirming school environments which are inclusive and supportive of student’s social, emotional, and cultural needs.
7. Provide key administrative, educator, and paraprofessional staff with the necessary training to recognize signs of changes in mental and physical health among students.
8. Provide Mental health gatekeeper training so that staff and peers take appropriate action when needed.
9. Support the mental health of all school personnel, including providing competitive wages, time off, access to well paid substitute teachers, regularly assessing staff well-being, and integrating measures to help personnel maintain their own empathy, compassion, and ability to create positive environments for students.
As superintendent and elected school board members, your roles include the evaluation of district operations, interpretations of public health policies, and health service delivery.
My role as a district resident is to help our district leadership identify the areas in need of protection, prioritization, and planning to keep Loveland City School District safe and in school: Universal Indoor Mask Requirements and adequate Mental Health Support for Students and Staff.
Signature
Add Additional Comment
References for Information:
https://www.scientificamerican.com/article/omicrons-effect-wont-be-as-mild-as-hoped1/https://www.reuters.com/world/us/us-coronavirus-cases-hit-record-high-2021-12-29/https://www.kcur.org/news/2021-12-17/kansas-city-hospitals-are-full-again-omicron-has-arrived-and-doctors-are-begging-for-your-helphttps://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7046a4-H.pdfhttps://www.the-scientist.com/news-opinion/omicron-propagates-70-times-faster-than-delta-in-bronchi-study-69540https://www.med.hku.hk/en/news/press/20211215-omicron-sars-cov-2-infectionhttps://edition.cnn.com/2021/12/28/health/chicago-childrens-hospital-surge-doctor-vaccines/index.htmlhttps://www.hhs.gov/sites/default/files/surgeon-general-youth-mental-health-advisory.pdfhttps://yourlocalepidemiologist.substack.com/p/our-youth-are-struggling-with-mental
Dr. Sherri Tenpenny testifies before the Ohio House Health Committee on June 8, 2021. During her presentation, she said vaccines are magnetizing to their recipients and “interface” with 5G cell towers. (Photo source: The Ohio Channel)
In June, Sherri Tenpenny, a state-licensed doctor of osteopathic medicine and notorious COVID-19 disinformer, baselessly claimed in a televised, government meeting that COVID-19 vaccines “magnetize” recipients and “interface” with cell towers.
The comment wasn’t an aberration from Tenpenny, who has in the past described vaccines as a tool of “depopulation.” The Ohio State Medical Board, an agency tasked with overseeing discipline and complaints of state physicians, still renewed her license in September as part what it called an “automatic” process of handling renewals.
Her renewal points to a bigger problem at the intersection of politics, mass media and public health: a loud, super minority of physicians has found ways to monetize lies about COVID-19 and vaccines that prevent it, and state medical boards are ill equipped to handle the problem, according to a report released earlier this month by the de Beaumont Foundation.
“During this ongoing public health emergency that has claimed more than 5 million lives globally, a small minority of physicians have exploited the credibility that comes with their medical licenses to disseminate disinformation to the public,” the report states. “Their lies, distortions, and baseless conspiracy theories have caused unnecessary suffering and death that are prolonging the pandemic.”
“Their lies, distortions, and baseless conspiracy theories have caused unnecessary suffering and death that are prolonging the pandemic.”
– de Beaumont Foundation
Only about 21% of state medical boards have taken any disciplinary action against a licensee for disseminating false or misleading health information, according to a survey conducted by the Federation of State Medical Boards. About 2 in 3 boards said they’ve noticed an increase in complaints on the issue.
Ohio’s medical board’s stated mission is to “protect and enhance the health and safety of the public through effective medical regulation.” Spokeswoman Jerica Stewart said state law allows the board to discipline doctors for making a “false, fraudulent, deceptive, or misleading statement in relation to the practice of medicine and surgery.” However, there’s a high standard of proof to meet. Tenpenny’s license, Stewart said, was automatically renewed, part of an automated process to keep up with the 92,000 licensees in Ohio. Tenpenny did not respond to an email.
“Ohio law prohibits the Medical Board from sharing details about received complaints and investigations even if a licensee chooses to publicly comment on their interactions with the board,” she said. “I’d also like to reiterate, a recent renewal does not prevent the board from taking future disciplinary action and does not mean that there isn’t an open investigation.”
The de Beaumont report criticizes boards that have “rubber stamped renewals for doctors who are in clear violation of medical standards, which allows them to do more harm with no questions asked.”
Medical boards have structural problems stopping them from disciplining disinformers, per the report. Their work is shrouded in secrecy, the problem is somewhat new and fast-evolving, and investigations are time consuming.
These claims fly in the face of real-world evidence showing vaccines are incredibly powerful protectors against serious health outcomes from COVID-19 like hospitalization or death. Likewise, researchers have found there’s no increase in mortality in vaccine recipients, and that recipients had lower rates of non-COVID-19 mortality after adjusting for age and other characteristics.
The de Beaumont Foundation, a public health advocacy group, commissioned polling on the issue from Morning Consult. Of 2,200 adult respondents, about 9 in 10 said physicians don’t have the right to “intentionally spread misinformation or false health information.” About 8 in 10 said they should be disciplined for doing so.
Ohio Governor Mike DeWine announced today that he has ordered the mobilization of an additional 1,250 members of the Ohio National Guard to support hospitals with the most critical needs across the state. The mobilization comes on the same day the state set an all-time high for the total number of COVID-19 hospitalizations during the pandemic.
The Ohio Hospital Association reported today that 5,356 people are currently hospitalized with COVID-19. One in four patients are COVID-19 positive. This surpasses the previous hospitalizations record of 5,308 on Dec. 15, 2020. Of today’s hospitalizations, 1,228 patients are in the ICU, which is approaching the record high of 1,318 ICU patients reported on Dec. 15, 2020.
While Southwest Ohio is not seeing the same volume of patients as northern parts of the state, Richard P. Lofgren, MD, President and Chief Executive Officer, UC Health, expressed concerns about the surge in cases making its way across the entire state during the coming weeks.
Ohio National Guard Deployment As hospitals struggle with staffing to support the surge in COVID-19 patients, Governor DeWine announced during a press conference today, that he has asked Major General John C. Harris, Jr., Adjutant General, Ohio National Guard, to mobilize an additional 1,250 members of the Ohio National Guard, bringing the total deployment of National Guard members working with Ohio’s healthcare systems to 2,300 members.
“This is not something we take lightly… We are asking them to leave their families, their jobs and homes. This is a huge sacrifice,” Governor DeWine said.
Governor DeWine previously authorized the deployment of 1,050 Ohio National Guard members on Friday, Dec. 17. Major General Harris said the Ohio National Guard’s goal is to augment hospitals’ medical staff and wraparound services. Teams including nurses and medics will provide clinical care and non-medical teams will offer support services such as food service, patient transportation within facilities, and administrative support.
Approximately 460 Guard members are deployed in the Cleveland area; more than 160 in the Toledo area; about 100 in Columbus area. Smaller numbers of the Guard will be deployed in the coming days in Mansfield, Dayton, and Lima to support hospitals. Guard personnel are also supporting testing sites in Cleveland and Akron.
“The National Guard has been indispensable,” said Robert Wyllie, MD, Chief Medical Operations Officer, Cleveland Clinic.
The Ohio Department of Health and the Ohio Hospital Association are working daily with Ohio hospitals to assess staffing needs to determine the most appropriate support from the Ohio National Guard.
“Everybody agreed when the decision was made to send in the National Guard to our hospitals … All the way through this, we are going to be guided by where they are needed most today. It should give people confidence that everybody is on the same page here. Let’s deploy them where they are needed the most,” Governor DeWine said.
Hospitals Hospitals have been taking extraordinary measures to manage this COVID-19 surge, including postponing elective surgeries, while battling staffing shortages as a result of COVID-19 infection or exposure, and burnout.
The northern parts of Ohio have been particularly hard hit, especially the greater Cleveland area, where one in three patients are COVID-19 positive, including ICU patients, according to OHA data.
“The hospital systems are under significant stress in Northern Ohio,” Dr. Wyllie said. “We are running 2,000 tests a day. Let me tell you about those tests: 36% of the people going into the Walker Center for testing are testing positive for COVID.”
The state’s strategic hospital zone and region structure has allowed hospitals to work together with neighboring hospitals to balance the load of patients. This structure continues to be vital as cases and hospitalizations dramatically rise statewide and staffing remains a significant concern.
While Southwest Ohio is not seeing the same volume of patients as northern parts of the state, Richard P. Lofgren, MD, President and Chief Executive Officer, UC Health, expressed concerns about the surge in cases making its way across the entire state during the coming weeks.
“Unfortunately, the pandemic is not over … we are seeing more cases now than we have ever seen along the way,” he said. “Now, the spread of Omicron is adding fuel to this raging fire. One of the things that I want to make sure that people understand, is that this not only affects the care of people with COVID, but also affects people who don’t have COVID. It squeezes out our ability to take care of patients with other life-serious or life-threatening problems, such as heart attacks and strokes.”
Governor DeWine also spoke with Jennifer Hollis, a critical care nurse at OhioHealth Riverside Methodist Hospital in Columbus, about her experience in the hospital.
“I just want everybody to be able to walk a mile in my shoes and kind of understand as a critical care nurse, what I am seeing when I am coming into work. It is beyond difficult,” Hollis said. “Our beds are full. There is nowhere else to go, and we are just as short-staffed as everyone else is seeing as well … We are tired, we are frustrated, and we want the best for all of our patients.”
Hollis urged Ohioans to get vaccinated to protect themselves, their loved ones, and their communities. “I’ll continue to fight for you, when you won’t fight for yourself. Please get vaccinated. Quarantine if you are symptomatic. Get tested,” she said.
Vaccination, prevention Governor DeWine emphasized that the COVID-19 vaccines remain a powerful tool to keep people out of the hospital. Since June 1, 2021, there have been 35,962 admissions, and 92.5% of those have been among people who are not fully vaccinated.
Now more than ever, it’s critical to follow prevention strategies including getting vaccinated, getting a booster shot if eligible, wearing face masks, washing your hands frequently, getting tested, and staying home if sick, even if symptoms are mild.
“We are looking now at an impact of COVID-19 that is unlike anything we’ve seen before in this pandemic,” said Bruce Vanderhoff, MD, MBA, Director, Ohio Department of Health. “We have access to a powerful tool that can really shield us from the worst outcomes of COVID-19, and that is vaccination.”
As of today, more than 6.9 million Ohioans have received at least their first dose of a COVID-19 vaccine. That’s 63% of those Ohioans eligible (ages 5 and older). More than 2.6 million have received an additional dose, or a booster dose.
Masking in Schools Today, the Ohio Hospital Association also distributed a letter from the Ohio Hospital Association and Ohio Children’s Hospital Association to Ohio school superintendents, administrators and school board members encouraging them to implement a masking requirement when students return from the holiday break. A masking requirement in schools will help limit community spread of COVID-19 and keep students in school, the letter said.
Holidays Dr. Vanderhoff encouraged Ohioans to celebrate safely this holiday weekend so we can all have a healthy start to 2022. “As we get ready to ring in a new year, please, think about the steps you can take to prevent COVID-19 spread before you gather. Keeping vaccinations up to date, appropriate testing, staying home if you feel the least bit sick, masking especially in crowded indoor environments, proper ventilation, and regular handwashing can all help prevent the spread of COVID-19, flu, and other illnesses this season,” he said.
An at-home COVID-19 test kit. Photo by Laura Olson, States Newsroom.
Washington, D.C. – State health officials on Thursday welcomed the Biden administration’s plan to require private health insurers to reimburse Americans for the cost of rapid, at-home COVID-19 tests — though the officials also raised questions about whether the process will be burdensome.
Making those tests more accessible will allow Americans to get results quickly and in the privacy of their own homes. That change may encourage more people to swab their nose when they first notice potential symptoms, experts from the Association of State and Territorial Health Officials told reporters.
“In this next phase of the pandemic, rapid access to rapid testing will be key,” said Dr. Nirav Shah, director of Maine’s Centers for Disease Control and Prevention, adding that it can help to combat potential surges and to pinpoint infections quickly so antiviral treatments can be used.
But several challenges could limit the impact of the cost reduction.
That includes lingering problems with sufficient supplies, uncertainty about the details of the reimbursement process, and questions about any potential effect on the data that’s reaching state and local health departments about infections in their communities.
Official guidance in January
Under the proposal that President Joe Biden announced Thursday, three federal departments — Health and Human Services, Labor and the Treasury — will issue official guidance by Jan. 15 that will detail what exactly private insurers must cover when it comes to rapid COVID-19 tests.
Those insurers already are required to pay for the PCR tests that must be sent to a laboratory for processing and take longer for results.
The upcoming change requiring insurance coverage of rapid, at-home tests, won’t be retroactive. That means Americans who have been shelling out roughly $25 for a package containing two of the popular Abbott BinaxNOW rapid tests can’t submit receipts for tests they’ve already purchased.
Other details of that requirement were unclear Thursday, including if there will be any limitations on the number of at-home tests that must be covered.
While the Biden administration has sought to reduce supply bottlenecks in producing those tests, Shah said some states are still having difficulty acquiring large volumes of the Abbott at-home tests.
That brand, which has been found to be highly accurate, has been relied on heavily even as more options have come on the market. Part of that demand comes from familiarity: Those administering tests in large settings have become familiar with their use.
What if you test positive?
Another challenge with increasing the use of at-home tests will be ensuring that individuals know what to do if they test positive.
Michael Fraser, ASTHO’s chief executive officer, said state health officials have been discussing whether those at-home tests should include an insert to help explain who to call and other next steps, so that contact tracing can occur.
“There is some concern that with the increase in at-home testing, getting those results reported to state health departments might be difficult, because the result doesn’t automatically go to public health authorities,” Fraser said.
However, there won’t be many results to get to state and local health officials if Americans with private insurance balk at fronting the money for tests while they await reimbursement.
Shah said a more accessible model would be to have individuals show their insurance card at a pharmacy as they would when getting a flu shot or picking up a prescription, rather than being charged at the register.
Having to pay for the tests, then wait for repayment, “introduces an access challenge for a lot of folks,” he said.
The Biden administration also plans to boost the number of free at-home tests distributed at community health centers and rural clinics, though those are intended to aid those who are not covered by private insurance.
A new bill specifying “blended learning” for the 2021-2022 school year has been approved by an Ohio Senate committee.
Senate Bill 229 is yet another bill meant to address the impact of the COVID-19 pandemic on student success and education, and was favorably passed in Senate Primary & Secondary Education Committee on Tuesday.
In the bill, school districts, including traditional public schools, STEM schools and community and charter schools, would have to have approval by the Ohio Department of Education to implement or discontinue a “blended learning model” by April 20, 2022. This is an extension of current law, which required the approval through July 1 of this year.
The blended learning model requires a school district to provide internet access and devices to each student using the model, and monitor and assess student achievement and progress while also communicating with parents or guardians about the progress.
A report must be submitted to the ODE by March 15 showing each school district’s total number of students in blended learning in 2021-22.
The bill also resets a measure passed through the budget bill, House Bill 110, which discounted standardized testing because of the pandemic’s disruption to education. Under current law, e-schools are required to disenroll a student who fails to take a state assessment for two consecutive years.
Under H.B. 110, that standardized testing rule was set aside and under the new bill, the exception would be extended through the 2022-2023 school year. This applies to any school who has an online school component.
Sen. Theresa Fedor, D-Toledo, accused legislators of creating the standardized testing amendment for e-schools as “problematic double-standard e-school favoritism.”
“If we’re going to provide flexibility and exemptions from standardized testing, it must be for all students no matter where they attend school,” Fedor said.
She brought up the latest court ruling requiring the defunct Electronic Classroom of Tomorrow (ECOT) to pay back $60 million in state funding it received after an investigation showed student engagement amounted to about an hour a day.
Fedor was the leader of a bill that attempted to change education laws in response to the pandemic, but her bill didn’t make it past the Ohio Senate.
She also attempted to add a provision to the blended learning bill on Tuesday that would allow public bodies, including school boards, to meet virtually if they chose to, but that measure was quickly tabled by the committee.
“I think people should be meeting in person,” state Sen. Andrew Brenner, R-Powell, the committee’s chair said. “I think that is pretty much what we’ve had conversations internally about, so I think we should leave it as it is.”
The amendment was tabled along party lines, but the bill itself was passed unanimously.