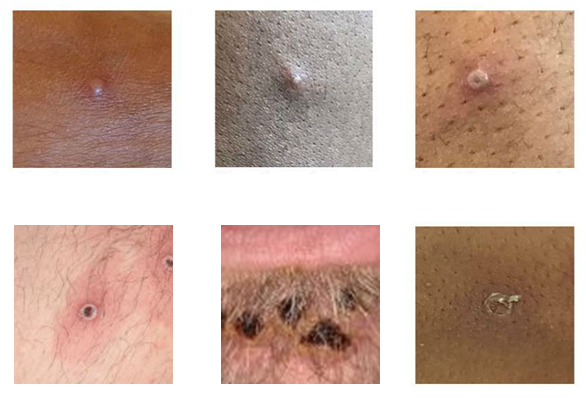
The monkeypox virus causes lesions that can resemble sores from acne, an ingrown hair or other viruses. They are infectious until the scab is fully healed. (UK Health Security Agency/CDC).
A Guest Column by Kenyon Farrow
It may come as a surprise to most people in Ohio that in addition to dealing with the ongoing problem of COVID-19 ebbs and flows of infections and variants, we actually have an entirely different infectious disease to be concerned about: monkeypox. And the Ohio Department of Health (ODH) has done very little else to engage the public in any detail about the virus, how it’s spread, any plans to scale up testing and when the state might be able to access the vaccines that are approved to prevent contracting the virus.
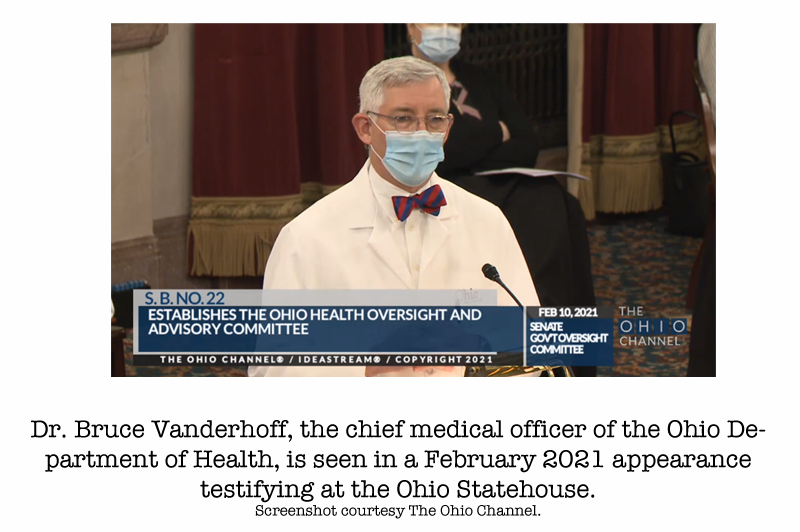
So far, all we’ve gotten is one press release announcing the first suspected case of monkeypox in the state. On June 13, the Ohio Department of Health issued a press release announcing this case, with messaging from ODH Director Dr. Bruce Vanderhoff, that seemed to downplay the threat monkeypox could play to the health of Ohioans.
“What I want to emphasize strongly is that monkeypox does not spread easily between people, and so the risk to Ohioans generally is very low,” he said.
Dr. Vanderhoff is correct in one sense. Monkeypox, compared to airborne virus like COVID-19, is less efficient in spreading from person to person. But it does spread through physical contact with someone who has contracted the virus — and that contact can be sexual contact, but also kissing, cuddling, bodily fluids and any contact where you could come into contact with the lesions that most often accompany an infection, and without testing can sometimes be mistaken for other diseases like herpes or congenital syphilis. And while monkeypox is rarely fatal, it is an extremely excruciating illness for those who contract it. Furthermore, it is more dangerous for infants and children, and pregnant people.
Since June 13, when the ODH first announced a suspected case, we now have 3 documented cases, according to the Centers for Disease Control & Prevention. While this number may seem low and like nothing most Ohioans should worry about, the truth is we actually do not have an accurate count to know whether monkeypox is spreading here, and how rapidly.
The ODH has not launched any public education materials in the form of televised or radio public service announcements, social media posts, press conferences or outreach efforts so most Ohioans would know about the virus, how its spread, and how to protect themselves. ODH has not announced any places around the state where one can get tested for monkeypox if you suspect you may have it.
And even if monkeypox cases here are currently few in number, they may not stay that way. Unlike COVID-19 where summertime has typically meant lower transmission rates because people are outdoors more and have windows open to allow clean air to circulate, there are more events where people come into close contact with one another. Airports and flights are packed. Summer is full of music festivals, county fairs, amusement parks and all sorts of events where people are often in close contact. Prisons and jails, due to medical neglect, overcrowding and unsanitary conditions created by lack of care, can also become a venue through which monkeypox could spread in and out of carceral settings.
Furthermore, monkeypox seems to be spreading rapidly in most American cities among LGBTQ people, particularly gay/bisexual men. June was Pride Month and every corner of the state has had pride festivals last month (and folks from Ohio, including myself, who’ve traveled to pride festivals in other cities and back) how do we actually know whether we have more cases without doing the proper public education and outreach campaigns connected to an infrastructure to offer testing to people who think they’ve been exposed?
JYNNEOS (also known as Imvamune or Imvanex) is a 2-dose vaccine for monkeypox currently in limited supply in the U.S., and according to the U.S. Health and Human Service’s (HHS) Office of the Assistant Secretary of Preparedness & Response, only 4 doses (enough for 2 people to be fully vaccinated against monkeypox) have been distributed to Ohio until more doses can be secured and imported later this year.
But will ODH or Gov. Mike DeWine advocate for Ohioans to get access to this vaccine once more doses become available? And will the set up a monkeypox testing and distribution plan?
I certainly hope so. But in the current political climate, it would not shock me if yet again good public health policy is taking a back seat to politics, endangering the lives of Ohioans in the process. The Ohio GOP’s in the last few years has passed anti-LGBTQ legislation, further criminalized abortion after the Supreme Court decision overturning Roe v. Wade, and their 2021 bill to dismantle the authority of the ODH to be able to issue and enforce measures to protect Ohioans during public health emergencies, all add up to ways in which ODH may have been the victim of state capture by personal and political interests that have zero to do with the stated mission of the organization.
One only need to look at what happened a month prior to the June notice on the first possible monkeypox case in Ohio—two ODH staffers (who were in the sexually transmitted infections prevention department) were fired or resigned because they included information about an upcoming training for medical providers on how to prescribe a medication used for women experiencing miscarriages or for abortions up to 10 weeks (which was 6 weeks before the U.S. Supreme Court decision to overturn Roe v. Wade) in an e-newsletter (first reported by Ohio Capital Journal on June 22).
The OCJ piece also noted that ODH’s HR department also took issue with the newsletters promotion of “National Masturbation Month; Honor Our LGBT Elders Day; International Day Against Homophobia, Pansexual and Panromantic Visibility Day; SLAM (Sexuality, Liberators, and Movers); Black and Blue – Suicide in our own Leather, Kink and Queer Communities; and National Condom Month.”
How is the STI prevention program at ODH supposed to do prevention work without taking advantage of these anniversaries to get the public’s attention? Is this the reason why they’ve been so lackadaisical about monkeypox virus education, outreach and testing?
To be sure, no one was looking for a monkeypox outbreak in 2022. As someone who’s worked in public health on infectious diseases as a policy advocate and journalist for more than two decades, this wasn’t on my radar either. But that’s the thing with infectious disease — they take advantage of human frailty and ignorance. And just when you least expect it, they’ve find a way to grow and to thrive. And ignorance on a virus and how to prevent it, and government negligence in creating educational, outreach, testing and vaccination opportunities become ways that diseases spread.
So knowing this, one would expect our state health department leadership to take more of an active role publicly to get ahead of what could be a real public health catastrophe. I hope they choose public health over politics.